| 신생아 정상 체온과 미숙 신생아 체온조절 |
Normal temperature of newborn infants and body temperature regulation in premature infants
사진 273.신생아들은 자신의 체온을 성숙하게 잘 조절하지 못하는 것이 보통이다.
특히 미숙아로 태어난 신생아들은 체온조절을 하는데 어려움이 많다.
체온을 정상적으로 유지하도록 신생아들에게 모자를 씌우고 옷을 따뜻하게 적절히 잘 입힌다.
포대기나 담요 등으로 적절히 잘 싸서 체온이 정상 이하로 떨어지지 않게 보호하고 양육한다.
때로는 어떤 이유로든 자신이 체온을 잘 조절할 수 없는 더 작은 미숙 신생아들이나 어떤 병을 앓는 신생아가 있으면 보육기 속에서 얼마동안 양육 치료하다가 클립으로 옮겨 양육치료하고 체온을 스스로 잘 조절할 수 있고 체중이 계속 증가하고 건강히 자라면 집으로 퇴원시키는 것이 보통이다.
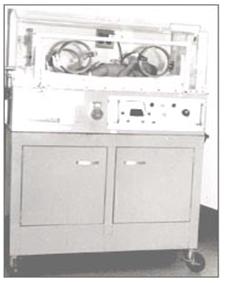
사진 274.어떤 병을 앓는 만삭 신생아들이나 체중이 아주 작은 미숙아들은 신생아기 이후 건강한 큰 아기들처럼 체온 조절을 스스로 잘 조절하지 못한다. 그들 스스로가 체온을 잘 조절 할 수 있을 때까지 필요에 따라 인큐베이터(보육기) 내에서 얼마동안 양육할 때가 많다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
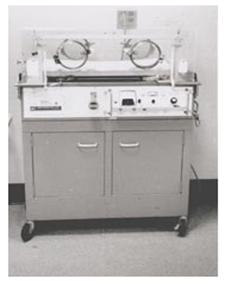
사진 275.만삭 신생아들, 특히 어떤 병을 앓는 신생아
들, 아주 작은 미숙아들은 신생아기 이후 건강한 아기들처럼 체온 조절을 스스로 잘 못한다. 이런 이유로 체온 조절을 스스로 잘 할 수 있을 때까지 미숙아를 인큐베이터(보육기) 내에서 양육하는 것이 보통이다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
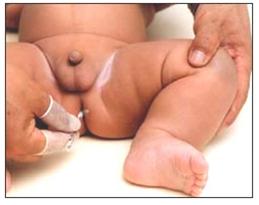
사진 276.아기 어디가 이상 한 것 같으면 항문 체온을 잰다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- 미숙 신생아들의 체온 조절 중추 기능은 만삭에 태어난 건강한 신생아의 체온 조절 중추 기능에 비해 덜 발육되어 있고 더 미숙하게 기능한다.
- 일반적으로 미숙아의 체표면적의 크기는 자신의 체중에 비하여 더 넓고 피하 지방 조직은 더 얇다.
- 이런저런 이유로 대부분의 미숙 신생아들은, 특히 아주 작은 저 체중 미숙 신생아들은 상당히 크게 성장할 때까지 스스로 체온 조절을 잘 못하는 것이 보통이다.
- 주위 온도가 갑작이 높아지면 미숙 신생아들의 체온도 주위 온도에 따라서 덩달아 올라가고 그와 반대로 주위 온도가 갑자기 내려가면 그들의 체온도 주위 온도에 따라 덩달아 내려갈 수 있는 것이 보통이다.
- 출생 시 체중이 2.5kg 이하 되는 미숙 신생아들이나 저체중 신생아들이 자기들 스스로 체온을 잘 조절할 수 있을 때까지 보육기 속에서 양육 받는 것이 일반적이다. 체온, 신생아 탈수 열 참조.
- 제 21권 소아청소년 가정간호 – 정상체온 비교표 표 3 참조
표 14. 나이(일령)에 따른 미숙 신생아와 만삭 신생아의 정상체온
|
출생체중 |
체중 1,500gm (3 lb, 5 oz) 이하 |
체중 1,501 gm~ 2,500 gm (3 lb, 5 oz ~ 5 lb, 8 oz) |
임신 36주 이상 2,500 gm (3 lb, 8 oz) 이상 |
|||||||||
|
나이 |
체온 섭씨 평균치±범위 |
체온 화씨 평균치±범위 |
체온 섭씨 평균치±범위 |
체온 화씨 평균치±범위 |
체온 섭씨 평균치±범위 |
체온 화씨 평균치±범위 |
||||||
|
1일 |
34.3 |
0.4 |
93.8 |
0.7 |
33.4 |
0.6 |
92.1 |
1.1 |
33.0 |
1.0 |
91.4 |
1.8 |
|
2일 |
33.7 |
0.5 |
92.7 |
0.9 |
32.7 |
0.9 |
90.9 |
1.6 |
32.4 |
1.3 |
90.4 |
2.3 |
|
3일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.4 |
0.9 |
90.4 |
1.6 |
31.9 |
1.3 |
89.4 |
2.3 |
|
4일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.3 |
0.9 |
90.2 |
1.6 |
31.5 |
1.3 |
89.6 |
2.3 |
|
5일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.2 |
0.9 |
90.0 |
1.6 |
31.2 |
1.3 |
88.1 |
2.3 |
|
6일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.9 |
1.3 |
87.6 |
2.3 |
|
7일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.8 |
1.4 |
87.4 |
2.5 |
|
8일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.6 |
1.4 |
87.5 |
2.5 |
|
9일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.4 |
1.4 |
86.7 |
2.5 |
|
10일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.2 |
1.5 |
86.4 |
2.7 |
|
11일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
29.9 |
1.5 |
85.8 |
2.7 |
|
12일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
29.5 |
1.6 |
85.1 |
2.8 |
|
13일 |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
29.2 |
1.6 |
84.6 |
2.8 |
|
14일 |
33.4 |
0.6 |
92.1 |
1.1 |
32.1 |
0.9 |
89.8 |
1.6 |
– |
– |
– |
– |
|
15일 |
33.3 |
0.7 |
92.0 |
1.3 |
32.0 |
0.9 |
89.6 |
1.6 |
– |
– |
– |
– |
|
4주 |
32.9 |
0.8 |
91.2 |
1.4 |
31.7 |
1.1 |
89.0 |
1.9 |
– |
– |
– |
– |
|
5주 |
32.1 |
0.7 |
89.8 |
1.3 |
31.1 |
1.1 |
87.9 |
1.9 |
– |
– |
– |
– |
|
6주 |
31.8 |
0.6 |
89.2 |
1.1 |
30.6 |
1.1 |
87.1 |
1.9 |
– |
– |
– |
– |
|
7주 |
31.1 |
0.6 |
87.9 |
1.1 |
30.1 |
1.1 |
86.2 |
1.9 |
– |
– |
– |
– |
출처 Standards and recommendations for Hospital Care of Newborn Infants, American Academy of Pediatrics. 5th, ed. p.91
Normal body temperature in newborns and thermoregulation of premature newborns
Normal temperature of newborn infants and body temperature regulation in premature infants
Picture 273. Newborns usually do not properly regulate their body temperature to maturity. In particular, newborns born prematurely have many difficulties in regulating body temperature. To maintain a normal body temperature, put a hat on the newborn and dress appropriately warmly.
Protect and nurture them by properly wrapping them in a blanket or blanket so that their body temperature does not fall below normal. Sometimes, if there are smaller premature newborns who cannot control their body temperature well for any reason or a newborn who has some disease, they are cared for a while in the incubator and then transferred to a clip for parenting treatment.
When they grow up healthy, they are usually discharged home.
Picture 274. Full-term newborns with certain diseases or premature infants with very small weights do not manage their body temperature as well as healthy older babies after a newborn. They are often brought up for some time in an incubator as needed until they can control their own body temperature. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 275. Full-term newborns, especially those with certain diseases, however, very small premature infants cannot regulate their body temperature as well as healthy babies after a newborn. For this reason, it is common to raise premature infants in an incubator until they can control their body temperature well. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 276. If something is wrong with the baby, measure the temperature of the anus. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
• The thermoregulatory centers of premature newborns are less developed and function more immaturely than those of healthy newborns born at full term.
• In general, the size of the body surface area of premature infants is larger than their body weight and the subcutaneous fat tissue is thinner.
• For one reason or another, most premature newborns, especially very small, low-weight premature babies, are usually not good at self-regulating their body temperature until they are quite large.
• When the ambient temperature suddenly rises, the body temperature of premature newborns also rises in accordance with the ambient temperature. Conversely, when the ambient temperature suddenly drops, it is common for their body temperature to drop along with the ambient temperature.
• It is common for premature or low birth weight newborns weighing less than 2.5 kg at birth to be reared in an incubator until they can control their body temperature. See body temperature, neonatal dehydration fever.
• Vol. 21 Home Nursing for Children and Adolescents – Refer to Table 3 of Normal Body Temperature Comparison Table
Table 14. Normal body temperature of premature and full-term neonates according to age (age)
표 14. 나이(일령)에 따른 미숙 신생아와 만삭 신생아의 정상체온
|
출생체중 birth weight |
체중 1,500gm (3 lb, 5 oz) 이하 weight 1500 gm (3 lb, 5 oz) or less |
체중 1,501 gm~ 2,500 gm (3 lb, 5 oz ~ 5 lb, 8 oz) Weight 1,501 gm to 2,500 gm (3 lb, 5 oz to 5 lb, 8 oz) |
임신 36주 이상 2,500 gm (3 lb, 8 oz) 이상 more than 36 weeks pregnant 2,500 gm (3 lb, 8 oz) or more |
|||||||||
|
나이 age |
체온 섭씨 평균치±범위 |
체온 화씨 평균치±범위 body temperature celsius Average ± range |
체온 섭씨 평균치±범위 body temperature celsius Average ± range |
체온 화씨 평균치±범위 body temperature Fahrenheit Average ± range |
체온 섭씨 평균치±범위 body temperature celsius Average ± range |
체온 화씨 평균치±범위 body temperature fahrenheit Average ± range |
||||||
|
1일 1 day |
34.3 |
0.4 |
93.8 |
0.7 |
33.4 |
0.6 |
92.1 |
1.1 |
33.0 |
1.0 |
91.4 |
1.8 |
|
2일 2 day |
33.7 |
0.5 |
92.7 |
0.9 |
32.7 |
0.9 |
90.9 |
1.6 |
32.4 |
1.3 |
90.4 |
2.3 |
|
3일 3 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.4 |
0.9 |
90.4 |
1.6 |
31.9 |
1.3 |
89.4 |
2.3 |
|
4일 4 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.3 |
0.9 |
90.2 |
1.6 |
31.5 |
1.3 |
89.6 |
2.3 |
|
5일 5day |
33.5 |
0.5 |
92.3 |
0.9 |
32.2 |
0.9 |
90.0 |
1.6 |
31.2 |
1.3 |
88.1 |
2.3 |
|
6일 6 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.9 |
1.3 |
87.6 |
2.3 |
|
7일 7 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.8 |
1.4 |
87.4 |
2.5 |
|
8일 8 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.6 |
1.4 |
87.5 |
2.5 |
|
9일 9 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.4 |
1.4 |
86.7 |
2.5 |
|
10일 10 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
30.2 |
1.5 |
86.4 |
2.7 |
|
11일 11 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
29.9 |
1.5 |
85.8 |
2.7 |
|
12일 12 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
29.5 |
1.6 |
85.1 |
2.8 |
|
13일 13 day |
33.5 |
0.5 |
92.3 |
0.9 |
32.1 |
0.9 |
89.8 |
1.6 |
29.2 |
1.6 |
84.6 |
2.8 |
|
14일 14day |
33.4 |
0.6 |
92.1 |
1.1 |
32.1 |
0.9 |
89.8 |
1.6 |
– |
– |
– |
– |
|
15일 15 day |
33.3 |
0.7 |
92.0 |
1.3 |
32.0 |
0.9 |
89.6 |
1.6 |
– |
– |
– |
– |
|
4주 4 week |
32.9 |
0.8 |
91.2 |
1.4 |
31.7 |
1.1 |
89.0 |
1.9 |
– |
– |
– |
– |
|
5주 5 week |
32.1 |
0.7 |
89.8 |
1.3 |
31.1 |
1.1 |
87.9 |
1.9 |
– |
– |
– |
– |
|
6주 6 week |
31.8 |
0.6 |
89.2 |
1.1 |
30.6 |
1.1 |
87.1 |
1.9 |
– |
– |
– |
– |
|
7주 7 week |
31.1 |
0.6 |
87.9 |
1.1 |
30.1 |
1.1 |
86.2 |
1.9 |
– |
– |
– |
– |
Source: Standards and recommendations for Hospital Care of Newborn Infants, American Academy of Pediatrics. 5th, ed. p.91
미숙 신생아들에게 모유나 인공영양을 먹일 때Breastfeeding or formula feeding for premature infants |

그림 277. 크고 건강한 미숙 신생아들에게는 모유를 보통으로 수유할 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D,. FAAP

사진 278. 아주 작은 미숙 신생아들에게 먹일 때 이런 종류의 특수 젖병으로 인공영양을 먹일 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- 출생 시 체중이 2~2.5kg이나 그 이상 되는 건강하고 큰 미숙아들에게 모유를 수유하는 방법이나 인공영양을 먹이는 방법은 만삭에 태어난 정상 신생아들에게 모유나 인공영양을 먹이는 방법과 별로 다른 것이 없다.
- 일반적으로 임신 35~37주에 태어난 비교적 큰 미숙아가 출생 후 대체로 건강하면 모유수유를 바로 할 수 있다.
- 출생 시 체중이 2kg이거나 그보다 더 작은 미숙아들이나 저체중 신생아들에게 모유를 수유 하거나 인공영양을 먹이는 데는 더 많은 먹이(피딩)는 식이 기술과 지식이 필요하다.
- 임신 35~37주경 태어난 미숙 신생아들 중 일부는 모유를 보통으로 잘 수유할 수 없을 때도 있다.
- 이 때 아기 스스로 엄마의 젖을 잘 빨아 먹을 수 있을 때까지 손으로 젖을 짜거나 유착기로 젖을 짜서 아기에게 먹일 수 있다.
- 게다가 출생 시 체중이 1.5kg 이하 되는 아주 작은 미숙 신생아들의 대부분은 엄마의 젖꼭지나 젖병 꼭지를 제대로 빨 수 있는 힘이 없을 때도 많다.
- 그래서 젖병 꼭지 구멍이 더 크게 뚫린 특수 젖병 젖꼭지로 인공영양을 먹일 때도 있고 그보다 더 쉽게 먹을 수 있게 만든 미숙 신생아용 특수 젖병을 이용해 인공영양을 먹일 수 있다.
- 때로는 손으로 짠 모유나 유착기로 짠 모유, 또는 인공영양을 피딩 튜브(듀브 영양)를 이용해서 아주 작은 미숙아들에게 먹이기도 하고, 짠 모유를 특별한 젖병 꼭지를 이용해서 젖병으로 먹이기도 한다.
- 모유는 소화가 비교적으로 잘 되고 감염병을 예방하는 데도 더 효과 있기 때문에 가능한 한 미숙아들에게 모유를 수유하는 것이 더 좋다.
- 대부분의 미숙 신생아들은 만삭 신생아들에 비해 엄마의 젖이나 인공영양을 먹은 후 잘 넘길 수 있다.
- 때로는 생리적 위식도 역류로 먹은 것이나 인공영양을 잘 넘길 수 있다.
- 또한 때로는 넘겨서 입안으로 올라온 위 내용물이 기관, 기관지, 폐 속으로 흡인되어 흡인 폐렴에 더 쉽게 걸릴 수 있다.
- 이런 저런 이유로 미숙 신생아들을 양호하는 데 더 많은 인내와 사랑, 보살핌이 필요하고 더 많은 육아지식이 필요하다.
- [부모도 반의사가 되어야 한다-소아가정간호 백과]-제 5권 인공영양 , 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방- 인공영양의 일정량의 칼로리 양에 따른 종류 (Kinds of infant formula by calories) 참조
Breastfeeding or formula feeding for very small premature infants
Breastfeeding or formula feeding for very small premature infants
- 태어난 날부터 엄마의 젖꼭지나 젖병 꼭지를 아기 스스로 잘 빨아 엄마의 젖이나 인공영양을 먹을 수 없을 정도로 아주 작은 미숙 신생아들도 있다.
- 아주 작은 미숙아(극소 저 출생 체중아)에게 모유나 인공영양을 보통으로 먹이면 대부분의 극소 저 출생 체중아들은 아주 미숙해서 스스로 엄마의 젖꼭지나 인공영양의 젖병 꼭지를 힘 있게 빨아먹을 수 없다.
- 이렇게 아주 작은 미숙아들에게는 태어난 날부터 10% 포도당액 혈관주사로 영양공급, 에너지와 수분을 공급해 주면서 미숙아가 스스로 엄마의 젖꼭지를 빨아 엄마의 젖을 먹을 수 있는지 바로 젖을 빨아 먹일 수 있는지 젖병 꼭지를 빨아 인공영양을 먹을 수 있는지 알아보는 것이 보통이다.
- 이 때 아주 작은 미숙 신생아들이 엄마의 젖꼭지나 젖병 꼭지를 힘 있게 빨아먹을 수 있으면 엄마의 젖을 먹이기 시작하든지, 미숙 신생아들이 쉽게 빨아먹을 수 있도록 특별하게 만든 젖병 젖꼭지로 인공영양을 먹일 수 있다.
- 그러나 아주 작은 미숙 신생아들의 대부분은 그들 스스로 젖꼭지를 빨아 모유나 인공영양을 먹을 수 없는 것이 보통이다.
- 만일 엄마의 젖꼭지를 잘 빨아 엄마의 젖을 먹을 수 있으면 아주 작은 미숙아에게 만삭 신생아에게 젖을 먹일 때와 거의 같은 방법으로 모유를 수유할 수 있다.
- 엄마의 젖꼭지나 젖병 젖꼭지를 빨아먹을 수 있는 힘도 없는 아주 작은 미숙 신생아들에게는 엄마의 젖이나 인공영양을 작은 비위 피딩 튜브로 먹이기도 한다.
- 이렇게 튜브 피딩을 하면서 때때로 젖병 젖꼭지를 빨려 인공영양을 먹여도 보고 엄마의 젖꼭지를 빨려 엄마의 젖을 먹여보기도 한다.
- 엄마의 젖꼭지나 젖병 꼭지를 힘 있게 빨아먹을 수 있는 미숙 신생아는 스스로 젖병 꼭지를 직접 빨아 인공영양을 먹도록 해 보고 엄마의 젖꼭지를 직접 빨려 엄마의 젖도 먹인다.
- 미숙 신생아가 스스로 엄마의 젖꼭지를 빨아 엄마의 젖이나 젖병 꼭지를 빨아 인공영양을 먹을 수 있고, 체중이 점점 정상적으로 계속 늘고 건강하게 성장발육하면 더 이상 피딩 튜브(튜브 영양법)로 먹이지 않는다.
- 미숙 신생아 스스로 엄마의 젖꼭지나 젖병 젖꼭지를 아기 입으로 직접 빨아 엄마의 젖이나 인공영양을 먹도록 한다.
- 그 이후에는 만삭으로 태어난 건강한 신생아들에게 엄마의 젖을 먹이는 방법과 인공영양을 먹이는 방법과 똑같이 미숙 신생아들에게 먹일 수 있다.
- 때로는 미숙 신생아들에게 인공영양을 쉽게 먹일 수 있게 만든 특수 젖병 꼭지로 인공영양을 먹일 수 있고 특수 인공영양을 먹일 수 있고 엄마의 젖꼭지에 가는 튜브를 부착시키고 그 튜브 끝부분과 엄마의 젖꼭지를 동시에 빨아 엄마의 젖도 먹고 그 튜브에서 나오는 짠 모유나 인공영양을 동시에 먹일 수도 있다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제 5권 인공영양, 비타민, 미네랄-특수 인공영양 참조.
- 아주 작은 미숙 신생아들에게 모유나 인공영양을 먹이는 방법의 한 예를 여기서 설명했다.
- 그때그때에 따라 아주 작은 미숙 신생아에게 모유나 인공영양을 적절하게 먹여야 한다.
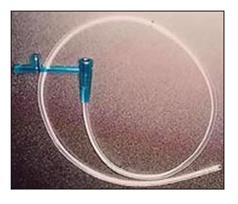
사진 279.피딩튜브:
아주 작은 미숙 신생아에게 짠 엄마의 젖(모유)을 먹일 때 특수 고무젖꼭지나 피딩튜브로 먹일 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
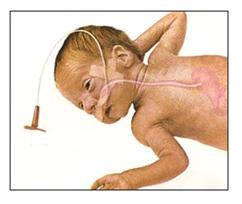
그림 280.아주 작은 미숙 신생아에게 짠 엄마의 젖(모유)을 먹일 때 특수 고무젖꼭지나 피딩튜브로 먹일 수 있다. 이런 피딩 튜브를 비위 피딩튜브라고 한다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 281.인공영양을 먹일 때 필요한 것들
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 282.인공영양을 먹일 때 쓸 수 있는 여러종류의 우유병들
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 283.저체중 신생아들이나 조숙아들에게 인공영양을 먹일 때 이용할 수 있는 특수 인공영양과 젖병 젖꼭지, 젖병.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
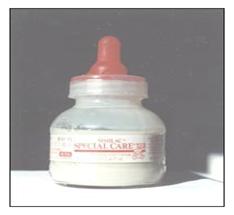
사진 284.만삭 신생아에게 인공영양이나 짠 모유를 먹일 때 이런 종류의 인공영양들을 사서 먹일 수 있다. 저체중 신생아들이나 조숙아들에게 먹일 수 있는 특수 인공영양.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
| 큰 미숙 신생아들에게 모유나 인공영양을 먹일 때 |
Breastfeeding or formula feeding for large premature infants
- 비교적 큰 미숙 신생아들에게 모유를 수유하는 방법과 인공영양을 먹이는 방법은 만삭에 태어난 정상 신생아들에게 모유나 인공영양을 먹이는 방법과 거의 같다.
- 임신 35~37주 사이 태어난 큰 미숙 신생아들의 대부분은 스스로 모유나 인공영양을 잘 먹을 수 있다. 우선 스스로 먹도록 시도해 보는 것이 좋다.
- 엄마의 젖꼭지나 인공영양 병 꼭지를 스스로 잘 빨아먹을 수 있고, 체중이 나날이 정상적으로 쑥쑥 늘면서 잘 성장발육하면 엄마의 젖이나 인공영양을 매 2, 3시간 간격으로 생후 약 2~3,4개월까지 먹이면 된다.
- 모유나 인공영양의 양은 체중과 나이(월령), 때로는 일령에 따라 조금씩 다르다.
- 젖을 잘 빨아먹지 못하는 경우, 엄마의 젖을 손으로 또는 유착기로 짜서 젖병에 담아 먹이든지 피딩 튜브로 먹일 수 있다.
- [부모도 반의사가 되어야 한다-소아가정간호 백과]-제4권 모유, 모유수유, 이유-젖 짜는 방법 참조.
- 체중이 적은 미숙 신생아들은 저 혈당증이나 탈수증에 더 잘 걸일 수 있다. p.00 신생아 저 혈당증 참조.
- 저혈당이 생기지 않게 예방하기 위해 생후 2~3시간부터 5% 포도당액 5~15cc 정도를 먹이기도 한다. 그 5% 포도당액을 먹고 아무 이상이 없으면 다음에는 인공영양을 먹여보기도 한다.
- 매번 인공영양을 먹일 때마다 미숙 신생아들이 먹는 양에 따라 다음 먹일 인공영양의 양을 점차로 늘린다. 2~3시간마다 하루 8~12번 먹인다.
- 처음 5% 포도당액을 먹인 후 매 1~ 2시간마다 5% 포도당액을 한두 번 시험 삼아 더 먹일 수도 있다.
- 이 때 5% 포도당액을 먹고 토하지도 않고 아무 이상이 생기지 않으면 다음 모유나 인공영양을 먹이는 방법도 있다.
- 그 후, 큰 미숙 신생아들에게 모유나 인공영양을 먹이는 방법은 만삭에 태어난 건강한 신생아들에게 먹이는 것과 거의 같다.
- 생후 3~4일 이후부터 엄마의 젖을 매 2~3시간 간격으로 자주 먹이면 된다([부모도 반의사가 되어야 한다-소아가정간호 백과]-제 4권 모유, 모유수유, 이유 참조).
- 먹는 양에 따라 인공영양의 양을 점점 더 늘린다.
- 인공영양을 먹일 때 구멍이 좀 더 크게 뚫린 젖병 젖꼭지를 이용하면 젖병 젖꼭지를 빠는 힘이 덜 들고 쉽게 인공영양을 먹을 수 있다.
- 만삭 신생아나 미숙아, 저체중 신생아에게 엄마의 젖을 먹이는 방법이나 인공영양을 먹이는 방법은 마치 약을 먹이는 것과 거의 같다.
- 그런데도 어떻게 그렇게 많은 자녀들을 낳고, 육아 공부도 안 했는데 그들을 모유 먹여 키웠는지 놀라울 지경이다.
- 먹이는 모유나 인공영양의 용량, 먹이는 간격, 먹이는데 요하는 시간, 먹이는 요령과 방법 등에 상당한 모유수유 식이 기술과 상식이 필요하다.
- 그렇지만 모든 부모들은 잘 해낼 수 있다는 자신감을 가져야 한다.

사진 285.아주 작은 조산아들이나 저체중 신생아들에게 보통 포물라의 칼로리 양보다 더 높은 고 칼로리 포물라를 먹일 수 있다. 고 칼로리 포물라 30cc에서 24칼로리의 열량이 나올 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

그림 286.큰 미숙 신생아들에게 모유수유하는 방법이나 인공영양을 먹이는 방법은 만삭 신생아들에게 모유수유하는 방법이나 인공영양을 먹이는 방법과 거의 같다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
| 미숙 신생아 양육과 보육기(인큐베이터) |
Premature infants and incubators
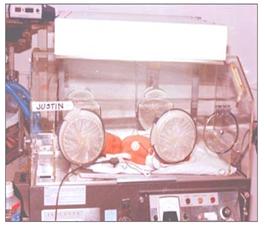
사진 287. 보육기 내에서 신생아 황달을 치료하고 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D.. FAAP
사진 288. 때로는 보육기 내에서 미숙 신생아(조산아)를 양육하고 병도 치료한다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- 만삭에 태어난 저체중 신생아들이나 미숙 신생아들이 스스로 체온을 잘 조절하지 못할 때나 만삭에 태어났지만 어떤 병을 앓는 신생아들은 자신의 체온을 정상적으로 스스로 잘 조절 할 수 없다.
- 아주 작은 미숙 신생아들, 어떤 병을 앓는 만삭 신생아들, 어떤 이유로든 신생아실에서 다른 신생들과 격리할 필요가 있는 신생아들, 어떤 이유로든 스스로 자기 체온을 적절히 조절해서 정상 체온을 유지할 수 없는 신생아들, 산소호흡 치료가 필요한 신생들, 습도조절이 필요한 신생아들을 위해, 또는 필요에 따라 한 병실에서 다른 병실로 신생아를 쉽게 이동할 수 있게 만든 작은 이동식 신생아실을 보육기 또는 인큐베이터라고 할 수 있다.
- 보육기 내 온도와 습도는 신생아의 체중, 나이, 건강상태 등에 적합하게 그때그때 조절해 줄 수 있다. 또 보육기 외부에 있는 박테리아이나 바이러스 등 병원체가 보육기 내에 있는 신생아에게 감염되지 않도록 하는 역할도 한다.
- 열고 닫을 수 있는 뚜껑이 보육기 맨 위에 있는 보육기,
- 열고 닫고 검진과 치료를 할 수 있게 옆에 문이 있는 보육기도 있고,
- 열고 닫을 수 있는 문이 앞뒤에 달린 보육기,
- 의사나 간호사가 손 팔을 집어넣고 보육기 속에 있는 신생아를 간호 치료해 줄 수 있는 큰 구멍이 보육기 앞에 있는 보육기 등 여러 종류의 보육기가 있다.
- 보육기 내 온도, 습도, 산소 농도 등은 그 안에서 치료와 양육 받고 있는 신생아의 나이(일령)나 질병, 체중 등에 따라 조절될 수 있다.
- 보육기 내 습도는 40~60%, 온도는 32~36℃ 정도 유지하고 신생아의 체온을 36~37℃ 정도로 유지시키는 것이 보통이다(표 15참조).
- 한 개 보육기 속에 한 명의 신생아가 있게 하는 것이 보통이다.
- 보육기를 한 번 쓴 후 다른 신생아에게 세균이 감염되지 않도록 살균처리한 후 다른 아기를 위해서 다시 쓸 수 있다.
-
저체중 신생아나 미숙 신생아, 또는 어떤 병을 앓는 신생아를 보육기 내에서 치료, 양육하다가 보육기 밖에서도 잘 성장 발육할 수 있으면 보육기 속에서 신생아 침대(아기 클립)로 옮겨 간호 양육하는 것이 보통이다.
When feeding premature infants with breast milk or artificial nutrition
Breastfeeding or formula feeding for premature infants
Figure 277. Breastfeeding can be done on a regular basis for large, healthy premature newborns. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 278. When feeding very small premature newborns, this type of special bottle can be given artificial nutrition. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
• Breastfeeding or artificial nutrition to healthy, large, premature infants weighing 2 to 2.5 kg or more at birth are not very different from methods of feeding breast milk or artificial nutrition to full-term newborns.
• In general, relatively large premature infants born between 35 and 37 weeks of gestation can breastfeed immediately after birth if they are generally healthy.
• More feeding dietary skills and knowledge are required to breastfeed or give artificial nutrition to premature infants or low birth weight newborns weighing 2 kg or less at birth.
• Some premature newborns born around 35 to 37 weeks gestation may not be able to breastfeed normally well.
• At this point, you can express your breast milk by hand or express your breasts with a breast pump until your baby is able to suck on her own milk and feed the baby.
• In addition, most of the very small premature newborns weighing less than 1.5 kg at birth often do not have the strength to properly suck the mother’s nipple or nipple.
• For this reason, artificial nutrition is sometimes given with a special bottle nipple with a larger hole in the nipple, and artificial nutrition can be fed using a special bottle for premature newborns that is easier to feed.
• Occasionally, hand-expressed milk, breast milk, or artificial nutrition is fed to very small premature babies using a feeding tube (tube nutrition) and expressed breast milk is fed from a bottle using a special bottle nipple.
• Breastfeeding is preferable to premature infants whenever possible, as breast milk is relatively easy to digest and is more effective in preventing infectious diseases.
• Most premature newborns are better able to pass after receiving mother’s milk or artificial nutrition than full-term newborns.
• Occasionally, physiological gastroesophageal reflux can easily pass through food or artificial nutrition.
• Also, sometimes the contents of the stomach that have been turned over into the mouth are aspirated into the trachea, bronchi, and lungs, making it more susceptible to aspiration pneumonia.
• For one reason or another, it takes more patience, love, care, and more parenting knowledge to take care of premature newborns.
• [Parents should also become at least the half-doctors – Encyclopedia of Pediatric Home Nursing] – Volume 5 Artificial Nutrition, Milk, Baby Food, Vitamins, Minerals, Protein, Carbohydrates, Fat – Types of artificial nutrition according to a certain amount of calories (Kinds of infant formula) by calories)
When feeding breast milk or artificial nutrition to very small premature newborns (extremely low birth weight premature infants/very low birth weight premature infants)
Breastfeeding or formula feeding for very small premature infants
• Some premature newborns are so small that from the day they are born, the baby cannot drink the mother’s milk or artificial nutrition by sucking the mother’s nipple or nipple from the bottle.
• When very small premature infants (very low birth weight infants) are fed breast milk or artificial nutrition on a regular basis, most very low birth weight infants are so immature that they cannot suck on their mother’s nipples or bottle nipples vigorously on their own.
• For these very small premature babies, from the day they are born, 10% glucose solution vascular injection provides nutrition, energy and moisture.
It’s common to find out if your baby can eat artificial nutrition.
• At this time, if very small premature newborns can suck on their mother’s nipples or bottle nipples vigorously, they can start breastfeeding or provide artificial nutrition with a specially designed bottle nipple for easy sucking by premature newborns.
• However, it is common for most of the very small premature newborns to suck on their mom’s nipples and not be able to get breast milk or artificial nutrition.
• If the mother’s nipples can be sucked well and the mother’s milk can be supplied, the very small premature infant can be breastfed in much the same way as a full-term newborn.
• Mother’s milk or artificial nutrition is sometimes fed through a small nasogastric feeding tube to very small premature newborns who do not have the strength to suck on the mother’s nipple or bottle.
• While doing tube feeding like this, sometimes suck the bottle nipple to give artificial nutrition or suck the mother’s nipple to feed the mother’s milk.
• Premature newborns who can suck their mother’s nipples or nipples vigorously, try to suck on their own nipples for artificial nutrition, and also feed the mother’s milk by directly sucking the mother’s nipples.
• If a premature newborn sucks on her mother’s nipples and sucks her mother’s milk or nipples for artificial nutrition, and her weight continues to grow and develops normally, she no longer feeds through a feeding tube (tube nutrition).
• Premature newborn herself sucks her mother’s nipples or bottle nipples directly into her mouth and lets them feed on her mother’s milk or artificial nutrition.
• After that, it can be fed to premature newborns in the same way that full-term healthy newborns are fed with mother’s milk and artificial nutrition is fed.
• Sometimes, artificial nutrition can be fed with a special bottle nipple that makes artificial nutrition easy to feed to premature newborns, and special artificial nutrition can be fed, and a thin tube is attached to the mother’s nipple, and the end of the tube and the mother’s nipple are inserted at the same time.
Your baby can suck it up and eat your mother’s milk, and you can feed squeezed milk or artificial nutrition from the tube at the same time. [Parents should also become at least the half-doctors – Encyclopedia of Pediatric and Family Nursing] – Volume 5 Artificial Nutrition, Vitamins, and Minerals – Refer to Special Artificial Nutrition.
• An example of how to feed breast milk or artificial nutrition to very small premature newborns is described here.
• From time to time, breast milk or artificial nutrition should be properly fed to very small premature newborns.
Photo 279. Feeding tube: Special feeding tubes can be used to feed very small premature newborns with the mother’s milk (breast milk). Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Figure 280. A special feeding tube can be used to feed a very small premature newborn with expressed mother’s milk (breast milk). Such a feeding tube is called a nasogastric feeding tube. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 281. What you need when feeding artificial nutrition/ Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 282. Various types of milk bottles that can be used for artificial nutrition. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 283. Special artificial nutrition and bottle nipples and bottles for use in feeding artificial nutrition to underweight newborns or premature infants. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 284. When feeding artificial nutrition or squeezed breast milk to a full-term newborn, you can buy these types of artificial nutrition and feed them. Special artificial nutrition that can be fed to underweight newborns or premature infants. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
When feeding large premature newborns with breast milk or artificial nutrition Breastfeeding or formula feeding for large premature infants
• The method of breastfeeding and feeding artificial nutrition to relatively large premature newborns is almost the same as the method of feeding breast milk or artificial nutrition to full-term newborns.
• Most of the large premature newborns born between 35 and 37 weeks of gestation are able to feed themselves well with breast milk or artificial nutrition. It’s best to try to eat it yourself first.
• If your baby is able to suck his mother’s nipples or the nipples of artificial nutrition bottles by yourself and grow and develop well with normal weight gain day by day, he can receive mother’s milk or artificial nutrition every 2 or 3 hours for about 2 to 3 or 4 months after birth.
• The amount of breast milk or artificial nutrition varies slightly depending on weight, age (month), and sometimes age.
• If suckling is difficult, the mother’s milk can be pumped by hand or with a bottled, or fed through a feeding tube.
• [Parents should also become at least the half-doctors – Encyclopedia of Pediatric and Family Nursing] – See Volume 4 Breastfeeding, Breastfeeding, Weaning – How to Express Milk.
• Premature newborns with lower weight may be more prone to hypoglycemia or dehydration. See Neonatal Hypoglycemia.
• In order to prevent hypoglycemia, 5~15cc of 5% glucose solution is sometimes given 2-3 hours after birth. If there is no problem after eating the 5% glucose solution, try artificial nutrition next time.
• Each time artificial nutrition is fed, gradually increase the amount of artificial nutrition for the next feeding according to the amount the premature newborns eat. Feed 8-12 times a day every 2-3 hours.
• After feeding the first 5% glucose solution, you may give more 5% glucose solution once or twice every 1 to 2 hours.
• At this time, if he eats 5% glucose solution and does not vomit and there is no abnormality, you can also feed the next breast milk or artificial nutrition.
• After that, feeding large premature newborns with breast milk or artificial nutrition is almost the same as feeding healthy newborns at full term.
• From the 3rd to 4th day after birth, you can feed his mother’s milk frequently every 2 to 3 hours ([Parents should also become at least the half-doctors – Encyclopedia of Pediatric and Family Nursing]-Vol. 4 Breastfeeding, Breastfeeding, Weaning).
• Gradually increase the amount of artificial nutrition according to the amount you eat.
• When feeding artificial nutrition, if you use a bottle nipple with a bigger hole, sucking force on the bottle nipple is less and you can eat artificial nutrition easily.
• Breastfeeding or giving artificial nutrition to full-term newborns, premature babies, or low-weight newborns is almost the same as giving medicines.
• Still, it’s amazing how they gave birth to so many children and breastfed them without even studying parenting.
• Considerable breastfeeding diet skills and common sense are required, such as the amount of breast milk or artificial nutrition to be fed, feeding interval, feeding time, and feeding tips and methods.
• However, all parents should have the confidence to do well.
Photo 285. Very small premature infants or underweight newborns can be fed a high-calorie formula that contains more calories than regular formula. 24 calories can come out of 30cc of high-calorie formula. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Figure 286. The method of breastfeeding or feeding artificial nutrition to large premature newborns is almost the same as that of breastfeeding or feeding artificial nutrition to full-term newborns. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Premature newborn care and incubator/ Premature infants and incubators
Photo 287. Treatment of neonatal jaundice in an incubator. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 288. Sometimes, premature newborns (premature infants) are raised and treated in an incubator. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
• When low-weight newborns or premature newborns born at full term do not control their body temperature well, or newborns who were born at full term but suffer from certain diseases cannot properly regulate their own body temperature.
• Very small premature newborns, full-term newborns with any illness, newborns who need to be isolated from other newborns in the neonatal unit for any reason, or who for any reason are unable to properly regulate their body temperature to maintain a normal body temperature. An incubator is a small mobile neonatal room that can be easily moved from one ward to another ward for newborns who need oxygen breathing therapy, or newborns who need humidity control.
• The temperature and humidity in the incubator can be adjusted at any time to suit the weight, age, and health condition of the newborn.
It also plays a role in preventing pathogens such as bacteria and viruses outside the incubator from infecting the newborn in the incubator.
• Incubators with an opening and closing lid on top of the incubator;
• There is also an incubator with a door next to it that can be opened and closed for examination and treatment;
• Incubators with front and rear doors that can be opened and closed;
• There are several types of incubators, such as incubators with a large hole in front of the incubator, through which a doctor or nurse can put their hands and arms in and nurse and treat a newborn in the incubator.
• Temperature, humidity, and oxygen concentration in the incubator can be adjusted according to the age, disease, and weight of the newborn baby being treated and cared for in the incubator.
• In the incubator, it is common to maintain a humidity of 40-60%, a temperature of 32-36℃, and a body temperature of a newborn baby of 36-37℃ (see Table 15).
• It is normal to have one newborn in one incubator.
• After using the incubator once, it can be used again for another baby after being sterilized so as not to infect other newborns.
• If low-weight newborns, premature newborns, or newborns with certain diseases are treated and raised in the incubator, and can grow and develop well outside the incubator, it is common to transfer them to a newborn bed (baby crib) in the incubator for nursing care.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2014 John Sangwon Lee, MD, FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.