신생아 뇌막염과 패혈증, Meningitis and sepsis in newborn infants (Neonatal sepsis)
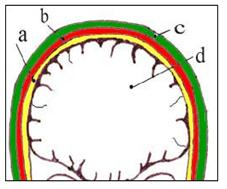
그림 155. 뇌막과 수막에 생긴 염증을 뇌막염 또는 뇌막염이라 한다. a-뇌막, b-두개골, c- 두피, d-뇌 Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
- 전신 혈액 박테리아 감염병을 패혈증이라 한다.
- 뇌막에만 생긴 박테리아 감염병을 박테리아 뇌막염이라고 한다.
- 신생아에게 생긴 패혈증을 신생아 패혈증,
- 신생아에게 생긴 뇌막염을 신생아 뇌막염이라고 한다.
- 박테리아가 신생아 피(혈액)에 감염되면 패혈증이 생길 수 있고, 신생아의 뇌막에 감염되면 신생아 뇌막염이 생길 수 있다.
- 신생아의 신체의 어떤 계통의 어떤 기관이나 조직에 박테리아 감염병이 1차로 생긴 후, 그 1차로 생긴 감염병을 일으켰던 박테리아가 전신 핏속을 감염되어서 전신 박테리아 감염병, 즉 패혈증이 이차로 생길 수 있다.
- 패혈증이나 균혈증을 일으킨 박테리아가 뇌막에도 감염되어 패혈증과 뇌막염이 동시 생길 수 있다.
- 박테리아 감염병이 신체의 어떤 계통의 한 기관이나 조직에 1차적으로 생긴 후 기관이나 조직에 국소적 감염병을 일으켰던 박테리아가 뇌막에 2차적으로 감염되어 신생아 뇌막염이 생길 수 있다.
- 박테리아 감염병 이외, 곰팡이(진균) 감염병, 기생충 감염병, 또는 바이러스 감염병이 전신에 생길 수 있다.
- 바이러스가 전신에 감염됐을 때 전신 바이러스 감염 또는 바이레미아라 한다.
- 곰팡이(진균)이 전신 핏속에 들어가 전신 곰팡이 감염병을 일으킬 수 있다.
- 일반적으로 박테리아 감염이 전신에 있는 피에 생겨 전신 박테리아 혈액 감염염을 패혈증이라고 하고 피 속에 박테리아가 있지만 아직도 감염병을 일으키지 않은 상태를 균혈증이라고 한다.
- 박테리아가 뇌막에 1차적으로 침입하여 뇌막에 감염되어 생긴 감염병을 뇌막염 또는 척수막염이라 한다.
- 신생아 패혈증을 일으킨 박테리아가 전신의 각계통의 핏속으로 퍼져 전신에 감염병을 일으키기도 하고 뇌수막에 침입해서 뇌막염을 일으킬 수 있다.
- 신생들, 특히 체중이 아주 작은 미숙 신생아들에게는 패혈증과 뇌막염이 동시 생길 수 있다.
- 신생아에게 패혈증이 있다고 의심하면 응급으로 요추천자를 해서 뇌척수 액을 뽑아 그로 그람 염색 현미경 세균 검사와 세균배양 등을 하고 그 세균에 의한 감염을 적절한 항생제로 치료한다.
- [부모도 반의사가 되어야 한다- 소아가정간호 백과]-제 7권 소아청소년 감염병-패혈증 참조.
- B군 용혈성 연쇄상구균, 대장균, 황색 포도상구균, 살모넬라, 시겔라, 리스테리아균 등 여러 종류의 박테리아 중 한 종류의 박테리아나, 때로는 한 종류 이상의 박테리아가 신생아에게 감염되어 신생아 패혈증 또는 뇌막염을 일으킬 수 있다.
- 특히 신생아는 박테리아 감염을 받을 때 그 박테리아 감염에 저항할 수 있는 저항력이 약하고 그 세균에 대한 면역성이 없거나 적어서 신생아에게 패혈증 또는 뇌막염이 동시 쉽게 생길 수 있다.
- 신생아들에게 패혈증이나 뇌막염을 잘 일으킬 수 있는 박테리아의 대부분은 신생아기 이후 영유아들이나 성인들에게 뇌막염이나 패혈증을 잘 일으키지 않는 박테리아도 있다.
| 다음 경우 신생아 뇌막염이나 패혈증이 생길 수 있다. |
- 분만 직전이나 분만 중, 또는 분만 직후 박테리아에 태반이나 양수, 또는 임신부나 분만부의 피, 소변, 대변 등을 통해 태아나 신생아가 감염될 수 있다.
- 불결한 신생아실, 집안, 또는 신생아를 돌보는 부모나 다른 사람들로부터 박테리아에 신생아가 감염될 수 있다.
- 출생 시 체중이 2kg 이하 저 체중 미숙 신생아들
- 분만 시작 24시간 전 양막 파수가 된 후 태어난 신생아들
- 뇌, 신장, 폐 등에 선천성 기형이 있는 신생아들
- 산모에게 융모양막염(Chorioamnionitis)이 있을 때
- 심폐소생술치료를 받은 신생아들
- 태변, 엄마의 변, 또는 피를 기도 속으로 흡인한 신생아들이 뇌막염 및, 또는 패혈증에 걸릴 기 쉽다.
- 분만부의 산도나 항문, 회음부에 B군 연쇄상구균 감염이 있을 때
| 신생아 뇌막염이나 패혈증의 증상 징후 |
- 신생아 뇌막염의 증상 징후는 뇌막염의 정도, 뇌막염과 패혈증이 동시 있는지, 뇌막염을 일으킨 세균의 종류, 합병증의 유무, 뇌막염의 진행 정도에 따라 다르다.
- 제대염, 신생아 농가진, 유방염, 결막염, 위장염, 폐렴, 중이염 등 국소적 감염병이 있으면서 신체의 한 계통의 국소 감염병을 일으켰던 세균에 의해 뇌막염 및, 또는 패혈증이 생길 수 있고 국소 감염병으로 생긴 증상 징후와 패혈증으로 인한 증상 징후가 동시 나타 날 수 있다.
- 신생아에게 생기는 패혈증의 아주 초기의 증상 징후가 특이하지 않고 포착하기가 어려워서 패혈증에 걸렸는지 확실히 모를 수도 있다.
| 다음은 증상 징후가 있으면 신생아 패혈증을 의심해야 한다 |
- 보통 때와 같이 잘 먹지 않고,
- 잠을 과도히 많이 자거나 잘 자지 않고,
- 창백하고,
- 원인을 확실히 알 수 없이 아기가 어딘가가 이상한 것같이 보이고,
- 미열 내지 고열이 나고,
- 몸이 차고,
- 구토 설사 등의 증상 징후가 초기에 나타나는 것이 보통이다.
- 뇌막염이나 패혈증을 앓는 신생아에게 나타나는 증상 징후는 신생아기 이후 영아들, 유아들, 학령기 아이들, 사춘기 아이들, 또는 성인들에게 생긴 뇌막염이나 패혈증의 증상 징후와 다른 점이 많다.
- 예를 들면 고열이 날 수 있다. 고열이 나는 대신 체온이 오히려 떨어져 몸이 찰 수 있고 저체온증이 생길 수 있다.
- 황달이 있을 수 있고,
- 점상 출혈,
- 피부 자반 등이 피부나 점막층에 나타날 수 있고,
- 피부 부종이 생길 수 있고,
- 피부 창백, 청색증이 나타날 수 있고,
- 계속 잠만 자기도 하고, 몸에 힘이 하나도 없이 몸이 축 늘어질 수 있다.
- 호흡수가 빨라지거나 가쁘게 숨을 쉴 수 있고,
- 무호흡증 등의 증상 징후가 있을 수 있다.
- 배가 불러질 수 있고,
- 구토, 설사를 하고
- 대변의 양이 줄어들기도 하고
- 소변의 양도 줄어들 수 있고
- 간 비대와 비장이 비대 되고, 식욕이 떨어져서 젖이나 인공영양을 전혀 먹으려 하지 않는 증상징후가 생길 수 있다.
- 몹시 보채기도 하고 전신 경련을 일으키기도 하고,
- 쇼크에 빠지고 적절히 속히 치료하지 않으면 짧은 시간 내에 사망할 수 있다.
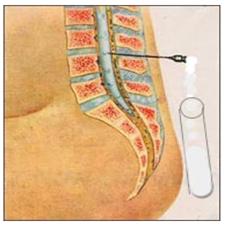
그림 156.요추천자로 얻은 뇌척수 액으로 뇌척수 액 혈구계산, 포도당 농도, 단백질 농도. 그람 염색 현미경 세균검사 및 세균배양 검사 등을 한다.
Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP

사진 157. 소변 검사 및 소변 세균 배양검사를 한다.
Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
| 신생아 뇌막염이나 패혈증의 진단 |
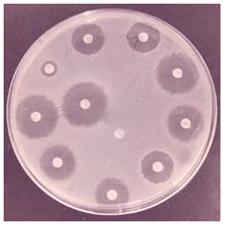
사진 158. 항생물질 감수성 검사.
뇌막염이나 패혈증이 의심되면 혈액, 소변, 대변, 뇌척수 액 등 피검물로 세균 배양검사를 한다. 세균 배양검사에서 나온 세균으로 항생물질 감수성 검사를 한다. Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
병력, 증상 징후, 진찰소견 등을 종합해서 뇌막염 및, 또는 패혈증이 있다고 의심되면 즉시 신생아 집중 중환자 치료실에 입원 진단 치료해야 한다.
- 가슴 X선 사진 검사 등으로 폐렴의 유무, 또는 심장 이상 등이 있나 알아본다.
- 소변, 혈액, 대변, 뇌 척수액 등 피검물로 그람 염색 현미경 검사, 현미경 세균검사, 세균 배양검사, 및 다른 여러 종류의 임상 검사를 해서 뇌막염 및, 또는 패혈증을 일으킨 원인균을 찾아 진단한다.
- C-반응성 단백 검사는 신생아 패혈증 조기진단에 많이 이용된다(출처; Contemporary Pediatrics, October 2009. p.52).
- 특히 저체중 신생 미숙 신생아에게 패혈증을 의심하면 요추천자로 얻은 뇌척수 액으로 단백질, 당 농도, 뇌척수 액의 백혈구 수, 적혈구 수, 유산탈수소 효소 농도, 뇌척수 액 검사를 하고 그람 염색 세균 현미경 검사 및 세균 배양검사 등을 해 진단 한다.
- 저체중 신생 미숙아에게 패혈증이 없이 뇌막염만 생길 수 있다.
- 또 뇌척수 액으로 진균검사도 동시 하는 것을 권장한다.
※포도상 구균(포도알균/Staphylococcus), 연구균(Streptococcus), 장구균(Enterococcus), 리스테리아균(Listeria) 등 12 균종 등으로 인한 균혈증이 시작한 후 불과 몇 시간 내 어떤 종류의 균으로 인해 균혈증이 생겼는지 진단 할 수 있는 Verigene Gram-Positive Blood Culture Nucleic Acid Test가 최근 미 FDA 승인을 받았다. 소스; Physician’s First Watch for June 29, 2012
표 6. 정상 뇌척수 액의 백혈구 수 Evaluation of normal cerebrospinal fluid WBC number
| 나이 | 백혈구 수/mcL | 다형핵호중구의 평균% |
| 미숙아 | 0-25 | 57% |
| 만삭아(생후 0-30일) | 7.3 +/- 13.9 (0-130) | 61-84% |
| 소아 | 0-7 | 5% |
표 7. 정상 뇌척수 액의 포도당 농도 Evaluation of normal cerebrospinal fluid glucose level
| 나이 | 관습 단위 | 에스 아이(SI) 단위 |
| 미숙아 | 24-63 mg/dL | 1.3-3.5 nmol/L |
| 만삭아 | 51.2 +/- 12.9 mg/dL | – |
| 소아 | 40-80 mg/dL | 2.2-4.4 nmol/L |
표 8. 정상 뇌척수 액의 포도당 농도/ 혈 중 포도당 농도 Normal cerebrospinal fluid glucose level/Blood glucose level
| 나이 | – | – |
| 미숙아 | 55-105% | – |
| 만삭아 | 44-128% | – |
| 소아 | 50% | – |
표 9. 정상 뇌척수 액의 유산탈수소효소 Lactic acid dehydrogenase in normal cerebrospinal fluid level
| – | – |
| – | 5-30 u/L (또는 혈청 치의 약 10%) |
표 10. 정상 뇌척수 액의 마이엘린 염기성 단백질 Myelin basic protein in normal cerebrospinal fluid (MBP)
| – | – |
| – | 4ng/mL 이하 |
표 11. 요척추 천자 개시 정상 뇌척수 액 압(옆으로 누워 있는 체위에서 요부 천자를 할 때)
Opening Pressure in lumbar puncture for normal cerebrospinal fluid
| 나이 | – | – |
| 신생아 | 8-11 cm H2O | – |
| 만삭아 | 20 cm H2O 이하 | – |
| 호흡에 따른 압의 변화 | 0.5 -1 cm H2O | – |
표 12. 정상 뇌척수 액의 단백질 Protein in normal cerebrospinal fluid
| 나이 | – | – |
| 미숙아 | 65-150 mg/dL | 0.65-1.5 g/L |
| 만삭아 | 64.2 +/- 24.2 mg/dL | – |
| 소아 | 5-40 mg/dL | 0.05-0.40 g/L |
출처 및 참조문헌;
-
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th& 19th edition, p.686
-
Neonatology Diseases of the fetus and infant, edited by Richard E. Behrman, p.528
-
Neonatology for the Clinician by Jeffrey Pomeranc and C. Joan Richardson, p.188
-
Growth and Development of Children, George H. Lowrey 8th edition
-
Nelson textbook, 15th, and 16th edition 그 외
| 신생아 뇌막염이나 패혈증의 치료 |
- 신생아에게 뇌막염 또는 패혈증이 있을 때, 또는 뇌막염과 패혈증을 동시 있을 때는 불과 1~2시간 사이에 생사를 결정할 정도로 심하게 앓을 수 있다.
- 이 병이 의심될 때는 즉시 신생아 집중치료실 입원 응급 치료를 받아야 한다.
- 뇌막염 및, 또는 패혈증을 일으킨 박테리아를 속히 죽일 수 있는 적절한 항생제를 경험적 선택 방법으로 골라 정맥주사 등으로 치료한다.
- 세균의 종류에 따라서 적절한 항생제를 선택해서 치료하는 것이 상당히 중요하다.
- 아기의 나이, 국소적 감염이 있으면 그 국소적 감염을 일으킨 세균의 종류, 원인균, 세균의 내성, 항생제 부작용 등을 고려해서 적절한 항생제를 선택한다.
- 예를 들면, 원인균을 확실히 알기 전 앰피실린(Ampicillin)과 젠타마이신(Gentamicin), 또는 밴코마이신(Vancomycin)과 크라포란 Claforan(Cefotaxime) 등 두세 가지 광범위 항생제 혈관주사 치료를 하다가 원인균을 확실히 알아낸 이후 그 원인균에 의한 감염병을 치료하는 데 가장 적절한 항생제로 10~21일 동안 치료하는 것이 보통이다.
- 패혈증이나 뇌막염을 일으키는 세균의 종류가 많고 사는 지역이나 나라에 따라 패혈증이나 뇌막염을 일으키는 세균의 종류가 다르고 항생제 내성이 수시로 생길 수 있기 때문에 심한 감염병을 치료할 때 항생제 선택은 항균제 감수성 검사의 결과와 주치의의 경험적 바탕에 따라 결정 하는 것이 옳다.
- 필요에 따라 산소호흡 치료, 포도당 전해질액 혈관주사, 보온 등으로 치료하고 증상 징후에 따라 대증 치료한다.
|
다음은 “저희 아가가 패혈증이래요”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q.&A. 저희 아가가 패혈증이래요..
Q.
먼저 주신 답변 많은 도움이 됐습니다. 감사드립니다.
태어난 지 12일 된 신생아이구요, 여자아기입니다..1주일정도의 검사결과 피 배양검사상에 균이 있다고 합니다.. 10일에 항생제를 바꿔서 치료를 시작했다구 하구요.. 3, 4일 뒤 결과가 나온다더군요.. 그리고도 3,4일은 더 치료를 해야 한다고 합니다.. 근데 전 궁금한 게 넘 많아서 주치의한테 여러 질문을 했지만 얻은 답변은 없습니다.. 주치의가 레지던트 2년차라는 것 같았어요..
제가 한 질문은 그 균이 심각한 균인지?? 그 균이 어떠한 균인지,, 균의 감염경로는 어떻게 되는지(예를 들어 피를 통한 감염인지 물로 인한 감염인지 등),, 정확한 치료기간은 어떻게 되는지(1주일정도 더 치료를 받아야 하지만 그 기간도 정확한건 아니라더군요)..
제가 질문을 이상하게 한 건가요… 제대로 답변을 안 주시더군요.. 어떻게 물어봐야 합니까?
그리고 패혈증도 바이러스과 박테리아이 있나요?? 면회 시 아기는 잘 먹고 열도 정상이며 몸무게도 출생 시 2.82kg이었는데 12일 후인 오늘3.12kg 라더군요.. 잘 성장하는 아기한테 균 감염이라니 이해가 되질 않습니다.. 그리고 잘 크는 아기라면 치료기간도 훨씬 단축되는 거 아닌가요?? 박사님의 답변 부탁드립니다.
A.
이청님께
안녕하세요. 좋은 질문해 주셔서 감사합니다.
아이의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등의 정보를 많이 알수록 답변을 드리는데 도움이 됩니다. 주신 정보를 토대로 해서 답변을 드리겠습니다.
Q.
그 균이 심각한 균인지??
A.
일부의 균혈증은 균혈증을 일으킨 세균이 아무런 치료 없이 체내 방어체계에 의해서 세균이 죽어 균혈증이 자연적으로 치료되는 경우가 있지만 대부분의 균혈증을 일으킨 세균은 혈류를 통해 뇌, 간, 폐, 심장, 신장 등 거의 모든 계통의 모든 기관들과 조직들로 퍼져 거기에 감염되고 전신 감염병을 일으킬 수 있습니다.
이렇게 전신 감염병 상태에 이르면 패혈증이라고 합니다.
아시겠지만 패혈증은 아주 무서운 감염병입니다.
여러 종류의 박테리아(세균)에 의해 패혈증이 생길 수 있고 그중 어떤 세균은 더 독성이 있고 독성이 많이 있는 세균 감염으로 패혈증이 생기면 불과 몇 시간 내지 하루 이틀 동안에 생명을 잃을 수 있습니다.
어떤 종류의 세균 독성은 약하기 때문에 패혈증이 여러 날 두고 생길 수 있습니다.
Q.
그 균이 어떠한 균인지,
A.
나이에 따라 패혈증이 생기기 전 이미 가지고 있는 건강 상태에 따라 패혈증을 일으키는 세균의 종류가 다를 수 있습니다.
Q.
균의 감염경로는 어떻게 되는지(예를 들어 피를 통한 감염인지 물로 인한 감염인지 등..),
A.
비강, 중이, 인두, 폐, 위장, 피부, 신장 등에 있는 1차 감염병 병소에 있던 세균이 혈액 속으로 들어가 2차적으로 패혈증을 일으키는 것이 보통입니다.
예를 들면 주사 맞은 상처, 못에 찔린 외상을 통해 세균이 혈액 속으로 들어가 1차적으로 패혈증을 일으키기도 합니다.
또 다른 예를 들면, 감기를 앓을 때 인두 점막층에 상주하고 있던 수막구균이 혈액 속으로 들어가 2차적으로 수막염과 수막균성 패혈증을 일으킬 수 있습니다.
신장염을 일으킨 대장균이 핏속으로 들어가서 수막염(뇌막염) 및, 또는 패혈증을 2차적으로 일으킬 수 있습니다.
피부에 생긴 농가진의 원인균 A군 베타 용혈성 연쇄상구균이 골수로 들어가서 골수염을 일으킬 수 있고 혈액 속으로 들어가서 2차적으로 패혈증을 일으킬 수 있습니다.
Q.
정확한 치료 기간은 어떻게 되는지(1주일정도 더 치료를 받아야 하지만 그 기간도 정확한건 아니라더군요)..
A.
패혈증을 일으킨 세균의 종류, 치료의 효과, 패혈증과 동시에 생겨있는 합병증 또는 치료의 결과 등에 따라 치료기간이 다릅니다.
심장내막염이 있고 패혈증이 있을 때는 여러 주 동안 항생제로 치료 합니다.
Q.
제가 질문을 이상하게 한건가요… 제대로 답변을 안 주시더군요.. 어떻게 물어봐야 합니까?
A.
질문하신 것은 잘못된 것 없고 이상한 것도 없고 당연한 것입니다.
이 세상에 완전한 사람은 하나도 없습니다.
의사도 완전한 사람이 아니고 또한 인간입니다.
엄마아빠도 완전한 사람이 아닙니다.
환자를 치료하는 의사도 가정을 가지고 있습니다.
의사 자신의 가정이나 개인 일로 남모르게 즐거운 때도 있고 개인적으로 불행한 일들도 의사에게 생길 수 있습니다.
환자를 내 몸과 내 가족같이 또는 그 보다 귀중한 분으로 알고 더 힘써 치료하는 중 사랑하는 환자가 죽어 마음이 몹시 아플 때도 있습니다.
가정에서 경제적으로 곤란을 받아 제대로 먹지도 못하고 환자를 사랑으로 돌보는 의사들도 있습니다.
인턴 수련을 받는 중 잠을 제대로 잘 시간이 없어 2-3일 동안 잠을 한잠도 자지도 못하고 환자를 돌 보아야 할 때도 있습니다.
의사가 사랑하는 엄마아빠 형제 누군가가 이 세상을 떠났지만 누구한테 위로를 받을 사이도 없이 환자를 보아야 할 때도 있습니다.
의사도 환자로부터 사랑과 동정과 격려를 받으면서 진료 활동을 한다면 얼마나 좋겠습니까?
보호자나 환아 자신이나 가족 또는 자녀에게 어떤 병이 났을 때 그 병을 치료 하는데 관해 조금도 공부하지 않고 치료를 받을 때 환자로서, 보호자로서 부모로서 책임져야 할 진료 부분에 관해서는 조금도 관심 갖지 않고 책임지지도 않고 치료 상 모든 것을 전적으로 의사에게만 의존하고 책임지라고 해서도 안 됩니다.
요령 있게 짤막하게 중요한 질문을 의사에게 해야 합니다.
또 그런 질문은 적절한 때에 적절하게 해야 합니다.
그리고 질문을 받을 수 있는 입장에 서 있을 때 해야 합니다.
대부분의 경우 의사는 한 환자만 보는 것이 아니라 숫하게 많은 환자들을 일정한 기간 동안 봐야 합니다.
그 중 어떤 환자는 초 분을 다투어 치료해야하는 긴급한 상황에 처해 있을 수 있습니다.
의사에게 시간이 있을 때 정중히 질문을 하십시오.
질문하시기 전에 상식적으로 알아야 할 의학지식은 도서관에서 공부해서 엄마아빠 스스로 배워야 합니다.
그런 의미에서 엄마아빠는 적어도 반의사가 되어야 합니다.
우리 의사들도 환자의 모든 병은 다 고칠 수 없고 환자들이나 보호자가 하는 모든 질문에 답변을 다 할 수 없습니다.
그러니 병명은 무엇이고 그 병은 무엇 때문에 생겼으며, 어떤 병들과 감별 진단을 하고 어떻게 구분하고 처방해 준 약명은 무엇이고 왜 그 약을 써야 하며 부작용은 무엇이고 그 약을 얼마동안 치료하고, 그 병의 예후는 어떻고 앞으로 어떻게 치료한다는 것을 설명해 주는 것이 의사의 의무이고 권리입니다.
환자가 질문하면 질문을 묵살하거나 딴전 피우거나 아예 화를 내는 의사 선생님도 가끔 있습니다.
의사들도 모든 환자나 보호자가 치료에 만족하기를 바랍니다.
그 나라 의료 정책, 그 병원의 의료 방침으로 각 의사가 인술을 베풀 수 없을 때도 많다는 것도 이해해 주셔야 합니다.
의사는 “환자에게 해를 끼치지 말라”라고 했지만 참말로 인술을 베풀기가 쉽지 않습니다.
Q.
그리고 패혈증도 바이러스과 박테리아이 있나요??
A.
많은 종류의 바이러스 감염병을 앓을 때 그 감염병을 일으킨 바이러스가 신체의 한 국소에만 국한되어 감염병을 일으킬 수 있고 때로는 혈액속으로 들어가 전신으로 퍼져 전신 바이러스 감염병이 생길 수 있습니다. 이런 경우를 바이레미아(Viremia)라고 합니다.
박테리아가 핏속에 있는 감염병을 박테레미아(Bacteremia) 또는 균혈증이라고 하고 그 박테레미아로 인해서 생긴 감염병을 패혈증(Septicemia)이라 합니다.
패혈증이 있을 때는 박테리아가 혈액 속에 있는 세포 즉, 혈구 등을 파괴시킬 수 있습니다. 그래서 패혈증이라는 말이 생긴 것일 것입니다.
Q.
면회 시 아기는 잘 먹고 열도 정상이며 몸무게도 출생 시 2.82kg였는데 12일 후인 오늘 3.12kg 라더군요. 잘 성장하는 아기한테 균 감염이라니 이해가 되질 않습니다.
그리고 잘 크는 아기라면 치료 기간도 훨씬 단축되는 거 아닌가요??
A.
물론 건강한 소아청소년들이나 성인들이 패혈증으로 불과 몇 시간 내 사망할 수 있습니다.
그러므로 패혈증이 완치될 때까지 병원에서 치료받는 것이 보통입니다.
패혈증을 일으킨 세균, 합병증 등에 따라 치료기간이 다릅니다.
더 자세한 치료기간에 관해는 의사 선생님에게 문의하시기 바랍니다. 패혈증, 뇌막염 등을 참조하고 [부모도 반의사가 되어야 한다–소아가정간호백과]-제 6권 신생아 성장 발육 양호 질환–신생아 뇌막염과 패혈증을 참조하시기 바랍니다.
질문이 더 있으시면 다시 연락해 주시기 바랍니다. 감사합니다. 이상원 드림
|
다음은 “2개월 된 아이의 고열과 패혈증”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 2개월 된 아이의 고열과 패혈증에 대해서..
Q.
안녕하세요..
저의 아이는 2개월 된 남자아이입니다. 5일전 밤에 고열이 있어서 다음날 병원에 갔습니다.
병원에 갔을 때는 열이 좀 내린 상태였고 혈액검사와 가슴 x-ray를 촬영했는데.. x-ray 소견은 정상이었고 혈액검사에서 백혈구 수치가 높게 나온다고 했습니다.
그날 소변검사를 하려고 했으나 못하고 해열제만 받아서 왔습니다.
저녁에 또 열이 나면서 아이가 끙끙 앓아서 해열제를 먹이고 주말이라 다른 병원 응급실로 갔습니다. 거기서 다시 혈액검사를 해봤는데 백혈구 수치가 더 많이 올라갔고 간기능과 관련된 검사 수치도 높고 염증지수도 상당히 높다고 했습니다.
패혈증이라고 하면서 원인을 알기 위해서 더 검사를 해봐야 한다고 했습니다.
그런데 그날 저녁부터 검사결과들이 나오기 전부터 항생제 치료를 했습니다.
거기서는 우선 기본적인 항생제 치료를 하고.. 균이 나오면 거기에 맞는 항생제를 쓴다고 하더군요.. 그리고 그 다음날.. 소변검사에서 백혈구가 많이 나온다고.. 하면서.. 소변을 통해서 감염이 된 것 같다고 하고.. 소변 균 배양을 해서 어떤 균인지 알아본다고 했습니다..
아직 배양결과는 안 나왔구요. 그리고 다음에 또 이런 감염이 되면 초음파 촬영을 해보자고 했습니다. 병원에서는 요로감염으로 생각하고 있는 것 같습니다.
아이는 열이 났다가 좀 내리기도 하고 열이 나고 보채는 것 외에는 크게 다른 증상 징후는 없습니다. 설사 구토 등도 없고 먹는 것도 괜찮고 그런데 처음에 갔던 병원의사에게 제가 응급실로 오게 되었다고 전화를 드렸는데 그 의사선생님은 항생제를 쓰기 전에 뇌척수 액 검사를 해서.. 뇌막염은 아닌지를 검사했어야 하는데 왜 안 했을까라고 말씀하시더군요.
제가 궁금한 것은 아이가 어떤 증상을 보인 때 뇌막염을 의심할 수 있는지요.
그리고 혈액 내에 백혈구 수치가 높고 염증지수가 높으면 균이 이미 혈액을 타고 전신으로 퍼졌다는 것을 의미하는지요. 그리고 요로감염이 원인이 되어서 패혈증 뇌막염이 올수 있는지요.. 그리고 항생제를 쓴 뒤에 소변을 받아 균 검사를 했는데 그래도 정확한 균배양이 되는지요.
소변균 검사에서 정확한 균이 검출되어서 거기에 맞는 항생제만 쓰면 완전히 치료가 되는 것인지 후유증은 없는 것인지 열이 난지 벌써 5일째인데 너무 늦은 것은 아닌지..
너무 걱정이 됩니다. 답변 부탁드립니다.
A.
오성님
안녕하세요. 좋은 질문해 주셔서 감사합니다.
아이의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등의 정보를 많이 알수록 답변을 드리는데 도움이 됩니다. 주신 정보를 토대로 해서 답변을 드리겠습니다.
Q.
“아이가 어떤 증상을 보인 때 뇌막염을 의심할 수 있는지요..”
A.
소아청소년이든지 성인이든 누구에든 열이 나면 의사들은 가장 먼저 뇌막염(사전에 수막염, 뇌막염이란 말을 쓰기 때문에 여기 뇌막염이란 말을 주로 쓰기로 합니다)으로 열이 나는지, 패혈증으로 열이 나는지 또는 다른 어떤 감염병으로 열이 나는지 항상 의심해 보는 것이 일반적입니다.
특히 생후 6개월 이전 영아들이나 신생아들에게 열이 나면, 고열이 나면서 독성 상태에 있으면, 뇌막염 및, 또는 패혈증을 일단 의심해 보는 것이 보통입니다.
박테리아 패혈증이나 박테리아 뇌막염을 앓는 아이들에게는 구토, 설사, 탈진, 탈수, 보챔, 고열, 창백, 자람증, 두통, 기민 등의 증상 징후가 있는 것이 보통입니다.
환아가 독성 상태에 빠져 있는(Toxic state) 것이 보통입니다.
독성 상태에 있다는 말은 남을 봐도 웃지 않고 엄마아빠에게도 웃지 않고, 먹지도 마시지도 않고, 또 잘 자지도 않고 혼자 놀려고도 하지 않고, 몹시 아파보이는 상태를 “톡식(Toxic)하다” 또는 “독성 상태에 있다“는 말을 씁니다.
Q.
혈액 내에 백혈구 수치가 높고 염증지수가 높으면 균이 이미 혈액을 타고 전신으로 퍼졌다는 것을 의미하는지요.
A.
일반적으로 열이 나면서 총 백혈구 수치가 상당히 높고 호중구 수가 비정상적으로 증가하면 세균성 감염병이 신체 어떤 계통 어떤 기관에 있을 가능성이 많습니다.
그러나 신체 어느 국소에 세균성 감염이 있는지는 확실히 말해주지 않습니다.
백혈구 수치가 비정상적으로 증가됐다고 해서 꼭 감염병이 있다 없다 항상 말할 수 없습니다.
백혈구 수치가 비정상적으로 낮을 때도 심한 감염병을 앓고 있을 수 있습니다.
백혈구 수치가 상당히 높을 때도 박테리아 감염병이 신체의 한 국소에만 경미하게 있을 때가 많습니다.
백혈구 수치가 낮더라도 박테리아가 혈액 속으로 이미 퍼져 패혈증이나 뇌막염에 걸려 있을 수 있습니다.
우리 몸 전 혈액에 박테리아가 있을 때도 있지만 우리 몸은 병원성 세균 침입에 대항할 수 있는 자연 방어 체계에 의해서 그런 세균 침입을 방어하기 때문에 패혈증에 걸리지 않는 때가 더 많이 있습니다.
Q.
그리고 요로감염이 원인이 되어서 패혈증이나 뇌막염이 올 수 있는지요..
A.
물론입니다. 올 수 있습니다. 1차 감염병의 병소가 요로에 있을 때 1차 감염병의 병소에 있던 세균이 전신 다른 계통의 어는 기관의 어느 국소에 감염될 수 있습니다.
Q.
그리고 항생제를 쓴 뒤에 소변을 받아 균검사를 했는데 그래도 정확한 세균배양이 되는지요.
A.
세균의 종류에 따라 다릅니다. 치료를 하기 위해서 쓴 항생제의 종류에 따라 소변 세균 배양의 결과가 다를 수 있습니다.
Q.
소변균 검사에서 정확한 균이 검출되어서.. 거기에 맞는 항생제만 쓰면.. 완전히 치료가 되는 것인지.. 후유증은 없는 것인지..
A.
요로 감염이 있는지, 요로 감염을 일으킨 세균은 어떤 종류인지, 왜 요로 감염이 생겼는지, 요로에 어떤 선천성 기형이 있는지 등을 알아보는 것이 중요합니다.
요로에 어떤 기형 또는 요로 감염의 정도에 따라 완치가 될 수도 있고 완치되지 않을 수도 있습니다.
어떤 병이든, 특히 뇌막염은 앓은 후, 후유증이 생길 가능성이 있습니다.
Q.
열이 난지 벌써 5일째인데.. 너무 늦은 것은 아닌지..
A.
소아청소년의 요로 감염은 호흡기 감염병의 다음으로 흔한 감염병 중 하나입니다.
요로 감염이 있을 때 적절한 항생제로 적절히 치료해도 열이 3-4일 동안 계속 날 수 있습니다.
너무 걱정하시지 말고 의사 선생님의 말씀대로 치료하시면 잘 나을 것입니다.
마치 제가 미국 소아청소년 학회에서 치른 소아청소년 전문의 시험 문제와 비슷한 아주 좋은 질문을 하셨습니다.
패혈증, 뇌막염, 세균(박테리아) 검사 참조.
[부모도 반의사가 되어야 한다–소아가정간호백과]-제 10권 소아청소년 신장 비뇨 생식기 질환–요로 감염, 소변검사.
제 13권 소아청소년 혈액과 림프 질환 및 종양–백혈구 수치.
제 21권 소아청소년 가정간호 및 학교건강–열 등을 참조하세요.
질문이 더 있으시면 다시 연락해 주시기 바랍니다. 감사합니다. 이상원 드림
- 병력, 증상 징후, 진찰소견 등을 종합해서 뇌막염 및, 또는 패혈증이 있다고 의심되면 즉시 신생아 집중 중환자 치료실에 입원 진단 치료해야 한다.
- 가슴 X선 사진 검사 등으로 폐렴의 유무, 또는 심장 이상 등이 있나 알아본다.
- 소변, 혈액, 대변, 뇌 척수액 등 피검물로 그람 염색 현미경 검사, 현미경 세균검사, 세균 배양검사, 및 다른 여러 종류의 임상 검사를 해서 뇌막염 및, 또는 패혈증을 일으킨 원인균을 찾아 진단한다.
- C-반응성 단백 검사는 신생아 패혈증 조기진단에 많이 이용된다(출처; Contemporary Pediatrics, October 2009. p.52).
- 특히 저체중 신생 미숙 신생아에게 패혈증을 의심하면 요추천자로 얻은 뇌척수 액으로 단백질, 당 농도, 뇌척수 액의 백혈구 수, 적혈구 수, 유산탈수소 효소 농도, 뇌척수 액 검사를 하고 그람 염색 세균 현미경 검사 및 세균 배양검사 등을 해 진단 한다.
- 저체중 신생 미숙아에게 패혈증이 없이 뇌막염만 생길 수 있다.
- 또 뇌척수 액으로 진균검사도 동시 하는 것을 권장한다.
※포도상 구균(포도알균/Staphylococcus), 연구균(Streptococcus), 장구균(Enterococcus), 리스테리아균(Listeria) 등 12 균종 등으로 인한 균혈증이 시작한 후 불과 몇 시간 내 어떤 종류의 균으로 인해 균혈증이 생겼는지 진단 할 수 있는 Verigene Gram-Positive Blood Culture Nucleic Acid Test가 최근 미 FDA 승인을 받았다. 소스; Physician’s First Watch for June 29, 2012.
Meningitis and sepsis in newborn infants (Neonatal sepsis) 신생아 뇌막염과 패혈증
Figure 155. Inflammation of the meninges is called meningitis. a-meninges b-cranium, c-scalp, d-brain Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
- A systemic blood bacterial infection is called sepsis.
- A bacterial infection that only occurs on the meninges is called bacterial meningitis. Newborn sepsis, neonatal sepsis, Meningitis in newborns is called neonatal meningitis. Infection of the bacteria into the newborn’s blood can lead to sepsis, and infection of the newborn’s meninges can lead to neonatal meningitis.
- After the first occurrence of a bacterial infectious disease in any organ or tissue of a certain system of the newborn’s body, the bacteria that caused the first infectious disease may infect the whole body blood, resulting in a second systemic bacterial infection, that is, sepsis.
- The bacteria that caused sepsis or bacteremia can also infect the meninges, causing sepsis and meningitis at the same time.
- Bacterial infectious disease may first occur in an organ or tissue of a certain system of the body, and then the bacteria that caused a local infectious disease in the organ or tissue may secondarily infect the meninges, resulting in neonatal meningitis.
- In addition to bacterial infectious diseases, fungal infectious diseases, parasitic infectious diseases, or viral infectious diseases can occur throughout the body. When the virus is infected systemically, it is called systemic viral infection or viremia.
- Fungi can get into the bloodstream and cause systemic fungal infections. In general, a bacterial infection occurs in the blood throughout the body, and systemic bacterial blood infection is called sepsis, and a condition in which bacteria are present in the blood but still does not cause an infectious disease is called bacteremia.
- Infectious diseases caused by bacteria first invading the meninges and infecting them are called meningitis or spinal meningitis.
- Bacteria that cause sepsis in newborns can spread into the blood of various systems throughout the body, causing infectious diseases throughout the body, and invading the meninges and causing meningitis. Sepsis and meningitis can develop at the same time in newborns, especially premature babies of very small weight.
- If it is suspected that the newborn has sepsis, an emergency spinal fluid is drawn out of the cerebrospinal fluid, and the gram staining microscopic bacterial examination and bacterial culture are performed, and the infection caused by the bacteria is treated with an appropriate antibiotic. [Parents should also be at least the half-doctors-Encyclopedia of Child and Family Nursing]-Vol. 7 Pediatric and Adolescent Infectious Diseases-See Sepsis.
- Group B hemolytic streptococcus, Escherichia coli, Staphylococcus aureus, Salmonella, Shigella, Listeria, etc.
- One type of bacteria, or sometimes more than one type of bacteria, can infect newborns and cause neonatal sepsis or meningitis.
- In particular, when newborns receive bacterial infections, they have weak resistance to resist the bacterial infection and have little or no immunity to the bacteria, so that the newborn can easily develop sepsis or meningitis at the same time.
- Most of the bacteria that can cause sepsis or meningitis in newborns are some bacteria that do not cause meningitis or sepsis in infants and adults after the neonatal period.
Neonatal meningitis or sepsis can occur in the following cases:
- The fetus or newborn can be infected with the placenta, amniotic fluid, or blood, urine, feces, etc. of a pregnant woman or childbirth immediately before, during, or immediately after childbirth.
- Bacteria can infect a newborn baby in an unclean newborn room, in the house, or from a parent or other person taking care of the newborn. Low-weight, premature infants weighing less than 2 kg at birth Newborns born after amniotic membrane rupture 24 hours before the start of delivery
- Newborns with congenital malformations in the brain, kidneys, and lungs.
- When the mother has chorioamnionitis
- Newborns receiving CPR treatment
- Newborns with meconium,
- mother’s stool or blood aspirated into the airways are susceptible to meningitis and/or sepsis.
- When there is group B streptococcal infection in the birth canal, anus, or perineum of the delivery part
Signs, symptoms of neonatal meningitis or sepsis
- Symptoms of neonatal meningitis differ depending on the degree of meningitis, whether meningitis and sepsis are present at the same time, the type of bacteria that caused meningitis, the presence of complications, and the progression of meningitis.
- Meningitis and/or sepsis may occur due to local infectious diseases such as omphalitis, neonatal impetigo, mastitis, conjunctivitis, gastroenteritis, pneumonia, otitis media, etc.
- Symptoms may appear simultaneously.
- The very early symptoms of sepsis in newborns are not unusual and difficult to detect, so you may not know for sure if you have sepsis.
Neonatal sepsis should be suspected
- if there are any signs, symptoms: your baby does not eat as well as usual,
- Sleeping too much or not sleeping well,
- Pale,
- The baby looks something weird without knowing the cause,
- Mild to high fever,
- The body is cold,
- Symptoms, such as vomiting, diarrhea, and the like are usually present early on.
- Symptoms in newborns with meningitis or sepsis differ in many ways from those of meningitis or sepsis in infants, school-age children, adolescent children, or adults after neonatal period.
- For example, your baby may have a high fever.
- Instead of having a high fever, the body temperature may drop, causing the body to become cold and hypothermia.
- There may be jaundice, petechiae, purpura of the skin may appear on the skin or mucous membrane layer, skin swelling may occur, pale skin, cyanosis may appear, Your baby can keep sleeping, and your baby body may be drooping without any strength in your body.
- You can breathe faster or breathe quickly, There may be signs of symptoms, such as apnea.
- The stomach can be full, vomiting, diarrhea The amount of stool decreases, The amount of urine can be reduced, Symptoms of an enlarged liver and an enlarged spleen, a loss of appetite, and not trying to eat milk or artificial nutrition at all can occur.
- It’s very unpleasant, sometimes causes systemic convulsions, shock can occur and die within a short period of time if not treated properly and quickly.
Figure 156. CSF blood count, glucose concentration, and protein concentration with cerebrospinal fluid obtained from a ureter.
Gram staining microscopic bacterial examination and bacterial culture examination, etc. are performed. Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP Picture
157. Urine tests and urine bacterial culture tests are performed.
Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
Diagnosis of neonatal meningitis or sepsis
Picture 158. Antibiotic susceptibility test.
If meningitis or sepsis is suspected, a bacterial culture test is performed with the specimens such as blood, urine, feces, and cerebrospinal fluid.
Antibiotic susceptibility tests are performed with bacteria from the bacterial culture test. Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
- If you suspect that you have meningitis and/or sepsis based on your medical history, symptoms, and medical examination findings, you should be admitted to the neonatal intensive care unit immediately and diagnosed.
- Check for pneumonia or heart abnormalities by examining a chest X-ray. Gram staining microscopic examination, microscopic bacteriological examination, bacterial culture examination, and various other types of clinical tests are performed with specimens such as urine, blood, feces, cerebrospinal fluid, etc. to find and diagnose the causative bacteria that caused meningitis and/or sepsis.
- The C-reactive protein test is widely used for early diagnosis of neonatal sepsis (source; Contemporary Pediatrics, October 2009. p.52).
- In particular, if you suspect sepsis in a newborn baby with low birth weight, protein and sugar concentration, white blood cell count, red blood cell count, lactate dehydrogenase concentration, cerebrospinal fluid, and Gram-stained bacterial microscopy and bacterial culture test are performed with cerebrospinal fluid obtained as a lumbar spinal fluid.
- Underweight newborn preterm infants can develop meningitis without sepsis. In addition, it is recommended to perform a fungal test with cerebrospinal fluid at the same time.
※ Diagnosis of what type of bacteria caused bacteremia within a few hours after the start of bacteremia due to 12 species such as Staphylococcus, Streptococcus, Enterococcus, and Listeria. The Verigene Gram-Positive Blood Culture Nucleic Acid Test, which is capable of being tested, has recently been approved by the US FDA. sauce; Physician’s First Watch for June 29, 2012
Table 6 Evaluation of normal cerebrospinal fluid WBC number 표 6. 정상 뇌척수 액의 백혈구 수
| Age | White blood cell count/mcL | Average % of polymorphonuclear neutrophils |
| Premature babies | 0-25 | 57% |
| Term infants ( 0-30 day) | 7.3 +/- 13.9 (0-130) | 61-84% |
| Children | 0-7 | 5% |
Table 7.Evaluation of normal cerebrospinal fluid glucose level 표 7. 정상 뇌척수 액의 포도당 농도
| Age | Customary Unit | SI units |
| Premature babies | 24-63 mg/dL | 1.3-3.5 nmol/L |
| Term infants | 51.2 +/- 12.9 mg/dL | – |
| Children | 40-80 mg/dL | 2.2-4.4 nmol/L |
Table 8.Normal cerebrospinal fluid glucose level/Blood glucose level 표 8. 정상 뇌척수 액의 포도당 농도/ 혈 중 포도당 농도
| Age | – | – |
| Premature babies | 55-105% | – |
| Term infants | 44-128% | – |
| Children | 50% | – |
Table 9. Lactic acid dehydrogenase in normal cerebrospinal fluid level 표9. 정상 뇌척수 액의 유산탈수소효소
| – | – |
| – | 5-30 u/L (or about 10% of serum level) |
Table 10. Myelin basic protein in normal cerebrospinal fluid (MBP) 표10. 정상 뇌척수 액의 마이엘린 염기성 단백질
| – | – |
| – | less than 4ng/mL |
Table 11. Opening Pressure in lumbar puncture for normal cerebrospinal fluid
표 11. 요척추 천자 개시 정상 뇌척수 액 압(옆으로 누워 있는 체위에서 요부 천자를 할 때)
| Age | – | – |
| Premature babies | 8-11 cm H2O | – |
| Term infants | 20 cm H2O 이하 | – |
| pressure can be changed according to respiration | 0.5 -1 cm H2O | – |
Table 12. Protein in normal cerebrospinal fluid 표 12. 정상 뇌척수 액의 단백질
| Age | – | – |
| Premature babies | 65-150 mg/dL | 0.65-1.5 g/L |
| Term infants | 64.2 +/- 24.2 mg/dL | – |
| Children | 5-40 mg/dL | 0.05-0.40 g/L |
Sources and references;
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th& 19th edition, p.686
- Neonatology Diseases of the fetus and infant, edited by Richard E. Behrman, p.528
- Neonatology for the Clinician by Jeffrey Pomeranc and C. Joan Richardson, p.188
- Growth and Development of Children, George H. Lowrey 8th edition
- Nelson textbook, 21st edition
- and others
Treatment of neonatal meningitis or sepsis
- When a newborn has meningitis or sepsis, or when meningitis and sepsis are present at the same time, it can be severe enough to determine life or death in only 1 to 2 hours.
- If you suspect this disease, you should be admitted to the neonatal intensive care unit immediately and seek emergency treatment.
- An appropriate antibiotic that can quickly kill the bacteria that caused meningitis and/or sepsis is empirically selected and treated with an intravenous injection. It is very important to select and treat an appropriate antibiotic according to the type of bacteria.
- If the baby has a local infection, the appropriate antibiotic is selected in consideration of the type of bacteria that caused the local infection, the causative agent, the resistance of the bacteria, and side effects of antibiotics.
- For example, before knowing the causative agent for sure, two or three broad-spectrum antibiotics such as Ampicillin and Gentamicin, or Vancomycin and Claforan (Cefotaxime) were treated, and the causative agent was clearly identified.
- After that, it is usually treated for 10 to 21 days with the most appropriate antibiotic for treating infectious diseases caused by the causative bacteria. \
- Since there are many types of bacteria that cause sepsis or meningitis, and the types of bacteria that cause sepsis or meningitis are different depending on the region or country in which you live, and antibiotic resistance can often occur, antibiotic selection when treating severe infectious diseases is the result of an antimicrobial susceptibility test and your baby’s doctor. It is correct to decide on an empirical basis.
- If necessary, treatment with oxygen respiration treatment, glucose electrolyte vascular injection, and warmth, and symptomatic treatment according to symptoms.
The following is an example of the online pediatric and adolescent health counseling question and answer on “My baby is sepsis”.
Q.&A.
- My baby is sepsis..
Q. The answer you gave first was very helpful. Thank you. I have a 12-day-old newborn baby, and I’m a baby girl.. As a result of the test for about 1 week, it is said that there are bacteria on the blood culture test.. The antibiotic was changed on the 10th to start treatment..
- The result is 3 or 4 days later. It is said that it comes out.. And it is said that you need to be treated for more than 3 or 4 days..
- But I had so many questions, so I asked several questions to my doctor, but I did not get any answers..
- It seemed that my doctor was a 2nd year resident.. The question I asked is is that a serious organism??
- What kind of fungus is the fungus, what is the path of infection of the fungus (for example, whether it is infection through blood or water, etc.), and how long is the correct treatment period (you need to receive treatment for a week or so, but the period is also It wasn’t accurate)…
- Did I make the question strange… he didn’t answer correctly..
- How should I ask? And is sepsis also virus and bacteria?? At the time of visit, the baby eats well, has a normal fever, and weighs 2.82 kg at birth, but today it was 3.12 kg 12 days later..
- It is not understandable that it is a fungal infection in a growing baby. And if it is a well-grown baby, the treatment period is much shorter. Isn’t it possible?? Please answer from the doctor.
A.
- Dear Lee Cheong Good morning. Thanks for the great question. The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided.
Q.
- Is that a serious one??
A.
- In some bacteremia, the bacteria that caused the bacteremia die without any treatment by the body’s defense system, and the bacteremia is naturally cured, but most of the bacteria that caused the bacteremia pass through the bloodstream to It can spread to all organs and tissues of all lines, infect them and cause systemic infectious diseases.
- This systemic infectious disease state is called sepsis. As you may know, sepsis is a terrifying infectious disease.
- Sepsis can be caused by several types of bacteria (bacteria), some of which are more toxic and more toxic bacterial infections that can kill lives in just a few hours to a day or two. Because some types of bacterial toxicity are weak, sepsis can develop over several days.
Q.
- What kind of fungus it is,
A.
- Depending on your age, the types of bacteria that cause sepsis may differ depending on the health conditions you already have before sepsis.
Q. What is the path of infection of the fungus (for example, whether it is an infection through blood or water, etc.),
A.
- It is common for bacteria from the primary infectious disease lesions in the nasal cavity, middle ear, pharynx, lungs, stomach, skin, and kidneys to enter the blood and cause secondary sepsis.
- For example, through an injection wound or a nail puncture trauma, bacteria may enter the blood and primarily cause sepsis.
- As another example, meningococcal resident in the pharyngeal mucosa when suffering from a cold can enter the blood and secondarily cause meningitis and meningococcal sepsis. E. coli, which caused nephritis, can enter the blood and cause meningitis (meningitis) and, or sepsis, secondarily. The causative agent of impetigo on the skin, group A beta-hemolytic streptococcus, may enter the bone marrow and cause osteomyelitis and may enter the blood and cause secondary sepsis. Q. What is the exact duration of the treatment (I need to receive treatment for a week or so, but the duration is not accurate)… A. Types of bacteria that caused sepsis
The following is an example of the online pediatric and adolescent health consultation question and answer on “High fever and sepsis in a 2-month-old child”.
Q&A
. About high fever and sepsis in a 2-month-old child..
Q.
Good morning.. My child is a boy who is 2 months old. I had a high fever the night before 5 days ago, so I went to the hospital the next day. When he went to the hospital, he had a little fever, he had a blood test and a chest x-ray.. The x-ray findings were normal and the blood test said he had high white blood cell counts.
That day, he tried to do a urine test, but he couldn’t, and he only got antipyretic. In the evening, the child got sick again, so I gave him antipyretic drugs and went to another hospital emergency room for the weekend.
I did a blood test there again, and the white blood cell count was higher, and the test level related to liver function was high and the inflammation index was quite high.
He said it was sepsis and that he had to do more tests to find out the cause. But from that evening, before the test results came out, I was treated with antibiotics.
There, he said that he would first take basic antibiotic treatment.. When bacteria come out, he said he would use the appropriate antibiotic..
And the next day..
While there were a lot of white blood cells in the urine test… he said that he was infected through urine..
They said that we could cultivate urine bacteria to find out what kind of bacteria they are…
The culture results haven’t come out yet. And next time I got an infection like this, I asked to do an ultrasound.
The hospital seems to be thinking of it as a urinary tract infection. The child may have a fever and then a little, and there are no signs of symptoms other than fever and fluff. I don’t have diarrhea, vomiting, etc. It’s okay to eat, but I called the hospital doctor I went to the first time that I came to the emergency room. It is. What I’m curious about is what symptoms can a child suspect of meningitis?
And if the number of white blood cells in the blood is high and the inflammation index is high, it means that the bacteria have already passed through the blood and spread throughout the body.
Also, is it possible for septic meningitis to come because of a urinary tract infection? And after using antibiotics, I received urine and tested for bacteria. In the urine bacteria test, the correct bacteria are detected, and if only the appropriate antibiotics are used, it will be completely cured or there will be no sequelae.
It has already been the fifth day after a fever, but is it too late? I’m so worried. please answer about my question.
A.
Oh Seong-nim Good morning.
Thanks for the great question. The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided.
Q. “When a child shows any symptoms, can he suspect meningitis…”
A. If anyone has a fever, whether a child or adolescent or an adult, doctors are the first to have a fever due to meningitis (meningitis, meningitis is used in advance, so I will mainly use the term meningitis here), whether a fever is caused by sepsis, or any other infectious disease. It is common to always question whether you have a fever. In particular, if infants or newborns before 6 months of age have a fever, if they have a high fever and are in a toxic state, it is common to suspect meningitis and/or sepsis.
Children with bacterial sepsis or bacterial meningitis usually have symptoms such as vomiting, diarrhea, exhaustion, dehydration, congestion, high fever, paleness, purpura, headache, and alertness. It is common for the child to be in a toxic state.
Saying that you are in a toxic state means that you do not laugh at others, do not laugh at your mom and dad, do not eat or drink, do not sleep well, do not try to play alone, and are “toxic” or “toxic” or “toxic”.
I use the phrase “I have.”
Q.
If the number of white blood cells in the blood is high and the inflammation index is high, it means that the bacteria have already passed through the blood and spread throughout the body.
A.
Typically, when you have a fever and your total white blood cell count is quite high and your neutrophil count is abnormally high, there is a good chance that a bacterial infection is present in some organ of the body. However, it does not tell for sure where the bacterial infection is in the body.
An abnormal increase in the white blood cell count cannot always tell that there is an infectious disease.
You may have a severe infectious disease even when your white blood cell count is abnormally low.
Even when the white blood cell count is quite high, the bacterial infection is often only mildly present in one area of the body.
Even if your white blood cell count is low, the bacteria can already spread into your blood and you may have sepsis or meningitis.
Sometimes there are bacteria in the blood all over our body, but there are more times when we don’t get sepsis because our body defends against such bacterial invasion by a natural defense system that can fight pathogenic bacterial invasion.
Q.
And is it possible that a urinary tract infection could cause sepsis or meningitis? A.
of course. Can come. When the lesion of the primary infectious disease is in the urinary tract, the bacteria in the lesion of the primary infectious disease may infect any part of the body in another system of freezing organs.
Q.
And after using antibiotics, I received urine and tested for bacteria, but is it still accurate bacterial culture?
A.
It depends on the type of bacteria. The results of urine bacterial culture may differ depending on the type of antibiotic used for treatment.
Q.
In the urine bacteria test, the correct bacteria are detected.. Would it be completely cured if only appropriate antibiotics were used.. Would there be no sequelae?
A.
It is important to find out if there is a urinary tract infection, what kind of bacteria caused the urinary tract infection, why there is a urinary tract infection, and what kind of birth defects there are in the urinary tract. Depending on the degree of urinary tract infection or any malformations in the urinary tract, it may or may not be cured. With any disease, especially meningitis, after suffering, there is a possibility that sequelae may occur.
Q.
It’s already been the fifth day since I’ve had a fever… Is it too late?
A.
Urinary tract infections in children and adolescents are one of the second most common infectious diseases after respiratory infections. When you have a urinary tract infection, fever can continue for 3-4 days, even if properly treated with appropriate antibiotics.
Don’t worry too much and you’ll be well treated as the doctor said. You asked a very good question, similar to the pediatrician exam questions I took at the American Academy of Pediatrics.
See sepsis, meningitis, bacteria (bacteria) test. [Parents should also be at least the half-doctors-Pediatric and Family Nursing Encyclopedia]-Volume 10 Child and adolescent kidney urogenital disease-Urinary tract infection, urine test. Volume 13 Pediatric and adolescent blood and lymphatic disease and tumor-white blood cell count. Refer to Volume 21, Child and Adolescent Family Nursing and School Health-Fever, etc. If you have more questions, please contact us again.
Thank you. Lee Sang-won dream If you suspect that you have meningitis and/or sepsis based on your medical history, symptoms, and medical examination findings, you should be admitted to the neonatal intensive care unit immediately and diagnosed.
Check for pneumonia or heart abnormalities by examining a chest X-ray. Gram staining microscopic examination, microscopic bacteriological examination, bacterial culture examination, and various other types of clinical tests are performed with specimens such as urine, blood, feces, cerebrospinal fluid, etc. to find and diagnose the causative bacteria that caused meningitis and/or sepsis.
The C-reactive protein test is widely used for early diagnosis of neonatal sepsis (source; Contemporary Pediatrics, October 2009. p.52).
In particular, if you suspect sepsis in a newborn baby with low birth weight, protein and sugar concentration, white blood cell count, red blood cell count, lactate dehydrogenase concentration, cerebrospinal fluid, and Gram-stained bacterial microscopy and bacterial culture test are performed with cerebrospinal fluid obtained as a lumbar spinal fluid.
Diagnose with your back. Underweight newborn preterm infants can develop meningitis without sepsis. In addition, it is recommended to perform a fungal test with cerebrospinal fluid at the same time.
※ Diagnosis of what type of bacteria caused bacteremia within a few hours after the start of bacteremia due to 12 species such as Staphylococcus, Streptococcus, Enterococcus, and Listeria.
The Verigene Gram-Positive Blood Culture Nucleic Acid Test, which is capable of being tested, has recently been approved by the US FDA. sauce; Physician’s First Watch for June 29, 2012 Table 6. Evaluation of normal cerebrospinal fluid WBC number Age White blood cell count/mcL Average% of polymorphonuclear neutrophils Premature babies 0-25 57% Term infants (0-30 days old) 7.3 +/- 13.9 (0-130) 61-84% Children 0-7 5% Table 7. Evaluation of normal cerebrospinal fluid glucose level Age Customary Unit S-I (SI) Unit Premature infants 24-63 mg/dL 1.3-3.5 nmol/L Term infants 51.2 +/- 12.9 mg/dL- Pediatric 40-80 mg/dL 2.2-4.4 nmol/L
Table 8. Normal cerebrospinal fluid glucose level/Blood glucose level age – – Premature infants 55-105%- Term infants 44-128%- Children 50%- Table 9. Lactic acid dehydrogenase in normal cerebrospinal fluid level — -5-30 u/L (or about 10% of serum level) Table 10. Myelin basic protein in normal cerebrospinal fluid (MBP)
Sources and references; The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th& 19th edition, p.686 Neonatology Diseases of the fetus and infant, edited by Richard E. Behrman, Neonatology for the Clinician by Jeffrey Pomeranc and C. Joan Richardson, Growth and Development of Children, George H. Lowrey 8th edition Nelson textbook, 15th, and 16th edition and others Treatment of neonatal meningitis or sepsis When a newborn has meningitis or sepsis, or when meningitis and sepsis are present at the same time, it can be severe enough to determine life or death in only 1 to 2 hours. If you suspect this disease, you should be admitted to the neonatal intensive care unit immediately and seek emergency treatment.
An appropriate antibiotic that can quickly kill the bacteria that caused meningitis and/or sepsis is empirically selected and treated with an intravenous injection. It is very important to select and treat an appropriate antibiotic according to the type of bacteria.
If the baby has a local infection, the appropriate antibiotic is selected in consideration of the type of bacteria that caused the local infection, the causative agent, the resistance of the bacteria, and side effects of antibiotics. For example, before knowing the causative agent for sure, two or three broad-spectrum antibiotics such as Ampicillin and Gentamicin, or Vancomycin and Claforan (Cefotaxime) were treated, and the causative agent was clearly identified.
After that, it is usually treated for 10 to 21 days with the most appropriate antibiotic for treating infectious diseases caused by the causative bacteria. Since there are many types of bacteria that cause sepsis or meningitis, and the types of bacteria that cause sepsis or meningitis are different depending on the region or country in which you live, and antibiotic resistance can often occur, antibiotic selection when treating severe infectious diseases is the result of an antimicrobial susceptibility test and your doctor’s doctor. It is correct to decide on an empirical basis.
If necessary, treatment with oxygen respiration treatment, glucose electrolyte vascular injection, and warmth, and symptomatic treatment according to symptoms.
The following is an example of the online pediatric and adolescent health counseling question and answer on “My baby is sepsis”. Q.&A. My baby is sepsis..
Q.
The answer you gave first was very helpful. Thank you. I’m a 12-day-old newborn baby, and I’m a baby girl.. As a result of the test for about 1 week, it is said that there are bacteria on the blood culture test.. The antibiotic was changed on the 10th to start treatment.. The result is 3 or 4 days later. It is said that it comes out.. And it is said that you need to be treated for more than 3 or 4 days..
But I had so many questions, so I asked several questions to my doctor, but I did not get any answers..
It seemed that my doctor was a 2nd year resident..
The question I asked is is that a serious organism?? What kind of fungus is the fungus, what is the path of infection of the fungus (for example, whether it is infection through blood or water, etc.), and how long is the correct treatment period (you need to receive treatment for a week or so, but the period is also It wasn’t accurate)…
Did I make the question strange… he didn’t answer correctly.. How should I ask? And is sepsis also virus and bacteria?? At the time of visit, the baby eats well, has a normal fever, and weighs 2.82 kg at birth, but today it was 3.12 kg 12 days later.. It is not understandable that it is a fungal infection in a growing baby. And if it is a well-grown baby, the treatment period is much shorter. Isn’t it possible?? Please answer from the doctor.
A.
Dear Lee Cheong Good morning. Thanks for the great question. The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided.
Q.
Is that a serious one??
A.
In some bacteremia, the bacteria that caused the bacteremia die without any treatment by the body’s defense system, and the bacteremia is naturally cured, but most of the bacteria that caused the bacteremia pass through the bloodstream to It can spread to all organs and tissues of all lines, infect them and cause systemic infectious diseases. This systemic infectious disease state is called sepsis. As you may know, sepsis is a terrifying infectious disease. Sepsis can be caused by several types of bacteria (bacteria), some of which are more toxic and more toxic bacterial infections that can kill lives in just a few hours to a day or two. Because some types of bacterial toxicity are weak, sepsis can develop over several days.
Q.
What kind of fungus it is,
A.
Depending on your age, the types of bacteria that cause sepsis may differ depending on the health conditions you already have before sepsis.
Q.
What is the path of infection of the fungus (for example, whether it is an infection through blood or water, etc.),
A.
It is common for bacteria from the primary infectious disease lesions in the nasal cavity, middle ear, pharynx, lungs, stomach, skin, and kidneys to enter the blood and cause secondary sepsis. For example, through an injection wound or a nail puncture trauma, bacteria may enter the blood and primarily cause sepsis. As another example, meningococcals resident in the pharyngeal mucosa when suffering from a cold can enter the blood and secondaryly cause meningitis and meningococcal sepsis. E. coli, which caused nephritis, can enter the blood and cause meningitis (meningitis) and, or sepsis, secondarily. The causative agent of impetigo on the skin, group A beta-hemolytic streptococcus, may enter the bone marrow and cause osteomyelitis, and may enter the blood and cause secondary sepsis.
Q.
What is the exact duration of the treatment (I need to receive treatment for a week or so, but the duration is not accurate)…
A.
The treatment period differs depending on the type of bacteria that caused sepsis, the effect of treatment, complications occurring at the same time as sepsis, or the result of treatment. If you have endocarditis and sepsis, you are treated with antibiotics for several weeks.
Q.
Did I make the question strange… he didn’t answer correctly.. How should I ask? A. The question you asked is nothing wrong, nothing strange, and it is natural. There is no one perfect man in this world. Doctors are not perfect people, they are also humans.
Mom and Dad are not perfect people either. Doctors who treat patients also have homes. There are times when the doctor’s own family or personal affairs are invisible, and personal unfortunate things can happen to the doctor.
There are times when a loved one dies and the heart hurts very much while trying harder to treat the patient as someone who is like my body and my family, or even more valuable.
Some doctors are unable to eat properly due to financial difficulties at home and take care of their patients with love.
During internship training, there are times when there is no time to sleep properly, so you cannot sleep for 2-3 days, and you have to take care of the patient.
There are times when a doctor loves a mother, a dad, a brother, and someone who has passed away, but you have to see a patient without anyone to comfort you.
Wouldn’t it be great if a doctor also received love, sympathy, and encouragement from the patient and practiced medical treatment? When a parent or guardian or child suffers from a disease, he or she does not study at all about treating the disease, and when receiving treatment, as a patient, as a parent, as a guardian, we do not care about the part of the treatment that we should be responsible for.
Nor should you be told to rely solely on your doctor for everything you care about and take responsibility for it. You should ask your doctor briefly important questions in a nutshell.
Also, such questions should be asked at the right time and at the right time. And do it when you are in a position to be asked questions.
In most cases, doctors need to see not only one patient, but a large number of patients over a period of time.
Some of them may be in an urgent need to treat them in seconds and minutes. Be polite to ask questions when you have time with your doctor.
Before asking questions, common-sense medical knowledge should be studied at the library and learned on your own. In that sense, mom and dad should at least be anti-doctors.
Even our doctors cannot cure every patient’s illness and cannot answer every question a patient or caregiver asks.
So, what is the name of the disease, what caused the disease, what is the name of the drug that has been differentially diagnosed, how to classify and prescribed it, what are the side effects, what are the side effects, and how long the drug is treated, and the disease.
It is the doctor’s duty and right to explain what is the prognosis for and how to treat it in the future. Sometimes doctors ignore the question, speak up, or even get angry when a patient asks a question.
Doctors also want every patient or carer to be satisfied with the treatment. It is important to understand that there are many times when each doctor is unable to provide Ninjutsu due to the country’s medical policy and the hospital’s medical policy. The doctor said,
“Do not harm the patient,” but it is really not easy to give ninjutsu.
Q.
And is sepsis also virus and bacteria?? A. When you suffer from many types of viral infectious diseases, the virus that caused the infectious disease is confined to one area of the body and can cause infectious diseases, sometimes entering the blood and spreading throughout the body, resulting in a systemic viral infection.
This case is called Viremia. An infectious disease in which bacteria are in the blood is called bacteremia or bacteremia, and an infectious disease caused by that bacteremia is called septicemia. In sepsis, bacteria
출처 및 참조문헌;
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2014 John Sangwon Lee, MD, FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.