신생아와 미숙 신생아의 분류, Newborn, classification of premature infants and low birth weight infants
| 신생아의 분류 |
1. 만삭 신생아(Term infants/Full term infants)
출생 시 체중의 크고 작음에 관계없이 임신 38주 첫날에서 부터 임신 43주 첫날 이전 임신기간 사이에 출생한 신생아
2. 과숙아(Postmature infants/Posterm)
출생 시 체중에 관계없이 임신 43주 첫날 이후(임신 294일 이후)에 출생한 신생아
3. 미숙아(Preterm/Preterm infants/Premature infants/조기산아/조산아)
마지막 월경을 시작한 날부터 임신 37주 첫날(임신 259일째) 마지막 시간 이전 출생된 신생아를 미숙아, 미숙 신생아, 조기산아 또는 조산아라고 한다.
미국 미숙 신생아(Preterm)의 출생률은 약 12.5%이다.
| 저 출생 체중아의 분류 |
1. 극소 저 출생 체중 신생아 Very low birth weight infants
미숙 신생아(미숙아)의 출생 시 체중이 1500g이거나 그 이하 되는 미숙 신생아를 극소 저 출생 체중아 또는 극소 저 출생 체중아라 한다.
극소 저 출생 체중아의 출생률은 1.5%이다.
2. 최 극소 저 출생 체중 신생아 Extremely low birth weight infants
미숙아의 출생 시 체중이 1000g이거나 그 이하 미숙아를 최 극소 저 출생 체중아 또는 최 극소 미숙아라고 한다. 출생률은 0.7%이다.
3. 저 출생 체중 신생아 Low birth weight infants
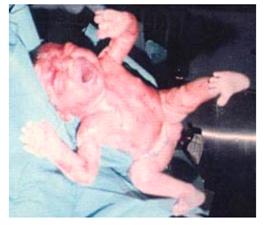
사진269.제왕절개 분만으로 태어난 미숙아
전신의 피부가 태지로 하얗게 덮여있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- 신생아의 출생 시 체중이 2.5kg 이하되는 미숙아나 만삭에 태어났지만 체중이 2.5kg 이하 되는 신생아를 통틀어 저 출생 체중아라고 한다.
- 미숙아와 저 출생 체중아(저 출생 체중 신생아)들을 양육할 때는 만삭에 태어난 신생아들을 양육할 때와는 달리 미숙아를 양육하는데 새로운 육아 지식과 상식이 더 많이 필요하다.
- 일반적으로 미숙 신생아들이나 저 출생 체중아들은 여러 가지 병에 더 잘 걸릴 수 있고, 그런 병에 걸리면 더 심하게 앓을 수 있는 것이 보통이다.
- 특히 극소 미숙아(Very low birth weight infants)와 미숙아의 출생 시 체중이 1000g 이하인 최 극소 미숙아 (Extremely low birth weight infants)를 양육하는 데 더 많은 건강문제가 생기고 양육비도 상당하다.
- 또 미숙아의 이환률도 상당히 높다. 예를 들면, 미국에서 연간 6600명의 뇌성 소아마비가 발생되고 그 중 40%는 저 체중 미숙아에 관련해서 생겼다고 한다. (참조 문헌; The New England Jounal of Medicine. April 17, 2008. vol 358 no 16).
- 또 저 체중 신생아들 스스로 모유나 인공영양을 경구로 잘 먹을 수 있고 스스로 체온을 잘 조절할 수 있을 때까지 일반 신생아실이나 특수 신생아실에서 특별히 양육해야 할 때가 많다.
- 한국에서 출생시 체중이 434g과 540g되는 최 극소 저 출생 체중아(Extremely low birth weight infants) 쌍둥이 자매가 건강하게 자라고 있다고 보도했다.
표 13. 임신 주수와 출생 시 체중에 따른 미숙아의 생존율
|
연구 년도 |
1987~1988년 |
1989~1990년 |
|
임신 주수에 따른 생존율 |
|
|
|
임신 제 23주 |
23 (0~33)% |
15 (0~29)% |
|
임신 제 24주 |
34 (10~57)% |
54 (27~100)% |
|
임신 제 25주 |
54 (30~72)% |
59 (27~74)% |
|
출생 체중에 따른 생존율 |
|
|
|
501~600 gm |
21 (0~44)% |
20 (0~33)% |
|
601~700 gm |
33 (9~50)% |
41 (25~56)% |
|
701~800 gm |
53 (31~73)% |
65 (38~83)% |
참조문헌; 미국 소아과 학회지 1996년 2월호에서 수집
| 미숙아와 저체중 신생아의 원인 |
① 임신부에게 어떤 병이 있어 임신 37주 전에 제왕절개수술 분만으로 태어난 신생아
② 어떤 원인으로 임신 37주 이전 자연분만으로 태어난 신생아
③ 임신부가 휴식을 충분히 취하지 못하거나 영양분을 충분히 섭취하지 못해서 임신 37주 이전에 태어난 신생아
④ 임신 중 심한 빈혈이나 영양실조, 또는 약물 중독에 걸린 임신부로부터 태어난 신생아
⑤ 자궁 기형이나 그 외 자궁 이상이 있는 임신부에게 태어난 신생아
⑥ 임신으로 생긴 임신 중독이나 그 외 여러 가지 질병을 앓는 임신부로부터 태어난 신생아
⑦ 임신부에게는 아무 이상이 없지만 쌍태 임신이나 다태 임신이 됐을 때
⑧ 또는 태아 자신에 어떤 이상이 있어 임신 37주 이전에 태어난 신생아
⑨ 그 외 다른 원인들

그림 270.쌍태 임신에서 저체중 신생아나 미숙아로 태어나기 쉽다
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- 미숙아나 저체중 신생아로 태어나는 원인들 중 가장 흔한 원인은 임신부가 임신 중 휴식을 충분히 취하지 못 했을 때.
- 통계에 의하면 직업여성이나 빈곤 가정 임신부, 또는 미성년 임신부에게 미숙아나 저체중 신생아가 태어날 수 있다.
| 미숙 신생아와 저체중 신생아의 치료와 양육 |
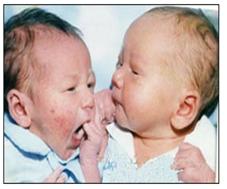
사진271.쌍태 신생아
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
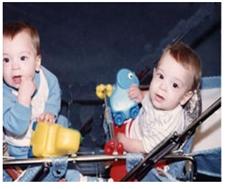
사진272.쌍태 영아
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- 세계 보건기구는 임신 38주 이후부터 임신 42주 이전 출생한 신생아를 만삭 신생아라고 정의한다.
- 임신 37주 이전 태어난 신생 신생아를 미숙아라고 한다.
- 미숙아나 저체중 신생아의 발병률과 사망률은 정상적으로 태어난 만삭 신생아의 것에 비해서 더 높다.
- 아주 작은 미숙아들이나 저 출생체중 신생아들의 대부분은 태어난 후 얼마 동안은 만삭에 태어난 신생아들과 거의 같게 모유를 수유할 수 없고 인공영양을 잘 먹을 수 없고 스스로 체온 조절을 잘 할 수 없다.
- 미숙아들은 병원체 감염에 대한 저항력이 약하고 감염병에 더 잘 걸릴 수 있고 걸리면 더 심하게 앓을 수 있다.
- 미숙아들이나 저체중 신생아들 스스로 젖이나 인공영양을 잘 빨아먹을 수 있고 체온 조절을 스스로 잘 할 때까지 신생아실에서 특별히 양육을 받다가 부모의 양육 하에서 집에서 잘 성장 발육할 수 있을 때 퇴원시키는 것이 보통이다.
- 미숙아들이나 저체중 신생아들이 태어날 때 입 안, 비강, 인두강 기도 내의 양수, 점액, 피 등을 흡입기나 흡입구로 흡입해서 숨을 잘 쉬도록 기도를 확보해야 한다.
- 큰 미숙아들이나 저 출생체중 신생아들이 태어났을 때는 만삭에 태어난 신생아들과 거의 마찬가지로 출생 시 기도 확보를 위한 처치를 하고 양육할 수 있지만
- 아주 작은 미숙아들이나 저체중 신생아들은 보다 더 적극적으로 특별히 치료받고 양육해야 한다. 출혈을 예방하기 위해 비타민 K 주사를 주고
- 임질균 결막염을 예방하기 위해 눈에 에리스로마이신 안약 등을 바르는 것은 만삭에 태어난 정상 신생아들에게 처치하는 것과 거의 마찬가지다.
- 미숙 신생아(미숙아)들이나 저체중 신생아들은 다음과 같은 점에 특별히 유의하면서 치료하고 양육해야 한다.
-
- 미숙아들의 체온 조절
- 미숙아들에게 모유를 먹일 때와 인공영양을 먹일 때
- 아주 작은 미숙아들에게 모유나 인공영양을 먹일 때
- 큰 미숙아들에게 모유나 인공영양을 먹일 때
- 미숙아와 보육기
- 미숙아와 습도
- 미숙아와 산소호흡
- 미숙아와 감염병 예방
- 미숙아 예방접종
- 미숙아 영양
- 미숙아 목욕
- 미숙아 양육 방법
| 미숙 신생아와 저체중 신생아의 예후 |
- 극소 미숙아(극소 저출생 체중아/Very low birth weight infants)의 단기간 건강‧양육 문제와장기간 건강‧양육 문제가 생길 수 있다.
- 황달, 저 혈당증, 빈혈, 두개강 내 출혈(두개골공 내 출혈), 저혈압, 동맥관 개존, 수혈, 수분 및 전해질 불균형, 신생아 괴사성 소장결장염, 무호흡증, 감염병, 영양공급 문제, 뇌 수종, 면역체 결핍증, 수정체 후 섬유증식증, 특발성 호흡곤란 증후군(유리질막증), 성장지연, 병원성 세균 감염병, 폐성 고혈압 등 단기간 건강‧양육 문제가 일시적으로 생길 수 있다.
- 천식, 성장지연, 세기관지염, 뇌성 마비, 성인 고혈압, 각막 이탈증, 근시, 사시, 알에스 바이러스 감염, 실명, 대뇌외축, 청력 감소, 기관지 폐 형성장애, 작은 창자 증후군, 반응성 기도 질환, 혈당 조절 기능 장애, 인슐린 저항 증가 등 장기간 건강‧양육 문제가 생길 수 있다.
Newborn, classification of premature infants and low birth weight infants 신생아와 미숙 신생아의 분류
Classification of newborns
1. Term infants/Full-term infants
Newborns born between the first day of 38 weeks and before the first day of 43 weeks of pregnancy, regardless of their weight at birth
2. Postmature infants/Posterm
Newborns born after the first day of 43 weeks of pregnancy (after 294 days of pregnancy), regardless of weight at birth
3. Preterm infants (Preterm/Preterm infants/Premature infants/Preterm infants/Premature infants)
Newborns born before the last hour of the first day of the 37th week of pregnancy (the 259th day of pregnancy) from the start of the last menstruation are called prematurity, premature newborns, premature babies, or premature babies.
The birth rate of preterm in the United States is about 12.5%.
Classification of low birth weight infants
1. Very low birth weight infants
Premature newborns (prematurity) who weigh 1500g or less at birth are referred to as very low birth weight infants or very low birth weight infants. The birth rate of very low birth weight babies is 1.5%.
2. Extremely low birth weight infants
Premature infants with a weight of 1000 g or less at birth are referred to as the lowest birth weight infants or the least premature infants. The birth rate is 0.7%.
3. Low birth weight infants
Picture 269: Premature infant born through cesarean section.
The whole body’s skin is covered in white. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- Premature infants weighing less than 2.5kg at birth or newborns born at full term but weighing less than 2.5kg are said to be low birth weight.
- When raising prematurity and low birth weight infants (low birth weight newborns), new parenting knowledge and common sense are required to raise premature infants, unlike when raising newborns born at full term.
- In general, premature newborns and infants of low birth weight are more susceptible to a number of diseases, and it is common for them to be more severely ill.
- In particular, raising very low birth weight infants and extremely low birth weight infants whose birth weight is less than 1000 g at birth poses more health problems, and childcare costs are significant. Also, the morbidity rate of premature babies is quite high.
- For example, 6600 cases of cerebral palsy occur annually in the United States, of which 40% are related to low-weight premature babies. (Reference; The New England Journal of Medicine. April 17, 2008. vol 358 no 16).
- In addition, low-weight newborns are often able to eat breast milk or artificial nutrients by themselves and need to be specially nurtured in a general neonatal room or a special neonatal room until they can control their body temperature well.
- It is reported that the twin sisters of extremely low birth weight infants, whose birth weights are 434g and 540g, are growing up healthy in Korea.
Table 13. The survival rate of premature infants according to gestational weeks and birth weight 표 13. 임신 주수와 출생 시 체중에 따른 미숙아의 생존율
|
Year of study |
1987~1988 |
1989~1990 |
|
Survival rate according to gestational weeks |
|
|
|
23rd week of pregnancy |
23 (0~33)% |
15 (0~29)% |
|
24th week of pregnancy |
34 (10~57)% |
54 (27~100)% |
|
25th week of pregnancy |
54 (30~72)% |
59 (27~74)% |
|
Survival rate by birth weight |
|
|
|
501~600 gm |
21 (0~44)% |
20 (0~33)% |
|
601~700 gm |
33 (9~50)% |
41 (25~56)% |
|
701~800 gm |
53 (31~73)% |
65 (38~83)% |
References Collection from the February 1996 issue of the American Journal of Pediatrics
Causes of prematurity and low birth weight newborns
① Newborns born with cesarean section surgery 37 weeks before pregnancy due to some disease in pregnant women
② Newborns born with natural delivery before 37 weeks of pregnancy for some reason
③ Newborns born before the 37th week of pregnancy because the pregnant woman did not get enough rest or ingested enough nutrients.
④ Newborns born to pregnant women with severe anemia, malnutrition, or drug addiction during pregnancy
⑤ Newborns born to pregnant women with uterine malformations or other uterine abnormalities
⑥ Newborns born to pregnant women suffering from pregnancy poisoning or other diseases caused by pregnancy
⑦ There is nothing wrong with pregnant women, but when they become twin or multiple pregnancies
⑧ Or a newborn baby born before the 37th week of pregnancy due to some abnormality in the fetus
⑨ Other causes
Figure 270: It is easy to be born underweight or premature in twin pregnancy. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- The most common cause of birth as prematurity or underweight newborn is when a pregnant woman does not get enough rest during pregnancy.
- Statistics show that pregnant women from working women, poor families, or underage pregnant women can have premature or underweight newborns.
Treatment and rearing of premature and underweight newborns
Picture 271. Twin newborns. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 272. Twin infants Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- The World Health Organization defines newborns born after 38 weeks of gestation and before 42 weeks of gestation as term newborns.
- Newborn babies born before 37 weeks of gestation are called premature babies. The incidence and mortality rates of premature or underweight newborns are higher than those of normal born full-term newborns.
- Most of the very small prematurity and low birth weight newborns cannot breastfeed for a period of time after birth, almost the same as those born at full term, cannot eat artificial nutrition well, and cannot control their body temperature well.
- Premature babies are less resistant to pathogen infections, are more prone to infectious diseases, and more severely ill if they do.
- It is common for premature infants and underweight newborns to receive special nursing in the neonatal room until they can suck on breast milk or artificial nutrients well on their own and control their body temperature well, and then discharge them when they can grow and develop well at home under parental care.
- When premature babies or underweight newborns are born, the airways should be secured so that they can breathe well by inhaling amniotic fluid, mucus, and blood in the mouth, nasal and pharyngeal airways through an inhaler or inhaler.
- When large premature babies or low birth weight newborns are born, they can be treated and nurtured to secure airways at birth, much like those born at full term. Very small premature babies and underweight newborns need to be treated and nurtured more actively and specifically.
- Give vitamin K injections to prevent bleeding
- Applying erythromycin eye drops to the eyes to prevent gonorrhea conjunctivitis is almost the same as treating normal newborns born at term.
Premature newborns (premature infants) or underweight newborns should be treated and nurtured, paying special attention to the following points.
- Control of body temperature in premature babies
- When breastfeeding premature babies and when feeding artificial nutrition
- When feeding breast milk or artificial nutrition to very small premature babies
- When feeding breast milk or artificial nutrition to large premature babies
- Premature babies and incubators
- Premature babies and humidity
- Premature infants and oxygen breathing
- Prevention of premature infants and infectious diseases
- Vaccination for premature infants
- Premature infant nutrition
- Premature baby bath
- How to raise a premature baby
- The prognosis of premature and underweight newborns
- Very low birth weight infants may have short-term health and parenting problems and long-term health and parenting problems.
- Jaundice, hypoglycaemia, anemia, intracranial hemorrhage (bleeding in the skull cavity), hypotension, arterial ductus, blood transfusion, fluid and electrolyte imbalance, neonatal necrotizing small bowel colitis, apnea, infectious disease, nutritional problems, hydrocephalus, immune system deficiency, lens
- Short-term health and rearing problems such as post-fibroproliferative disorder, idiopathic respiratory distress syndrome (vital dystrophy), growth retardation, pathogenic bacterial infection, and pulmonary hypertension may occur temporarily. Asthma, growth retardation, bronchiolitis, cerebral palsy, adult hypertension, corneal aberration, myopia, strabismus, RS virus infection, blindness, cerebral extraversion, hearing loss, bronchopulmonary dysplasia, small bowel syndrome, reactive airway disease, blood sugar control function Long-term health and parenting problems, such as disability and increased insulin resistance, can occur.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
-
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.